|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 2, No 1:22-25 © 2002
All rights reserved. Published by Pro Otology Association
Tos Technique (Modified Combined-Approach Tympanoplasty) and Reconstruction with Palisade Cartilage
Cem Uzun
Department of Otolaryngology, Medical Faculty, Trakya University, Edirne, Turkey
ABSTRACT
Objective: The aim of the present work is to describe one of the surgical techniques for cholesteatoma treatment, modified combined-approach tympanoplasty (Tos technique), and also to describe reconstruction of the tympanic membrane with palisade cartilage for to prevent postoperative retractions.
Study Design: The technique was described step by step. All operations were recorded on videotapes.
Setting: Operations were performed in the Department of Otolaryngology, Trakya University, Edirne, Turkey.
Technique: Tos technique consists of following steps: 1) Transcanal and retroauricular incisions; 2) transcanal posterior tympanotomy; 3) drilling of the postero-superior bony annulus; 4) transmeatal atticotomy; 5) transcortical intact canal wall mastoidectomy; 6) reconstruction of the attic and the tympanic membrane.
The cartilage for reconstruction of the attic and the tympanic membrane was taken from the concha. The perichondrium was preserved on one side of the cartilage, and half- to one-millimeter thickness slices were cut by scalpel. Cartilage palisades were placed according to Heermann's technique.
Patients: Three patients were operated on the technique, which was described above, between July 2001 and January 2002.
Intervention: Each patient underwent a thorough otolaryngologic (including oto-microscopic examination), audiologic (pure tone audiometry) and radiologic (mastoid X-ray and/or computed tomography) examination prior to surgery. All patients have been examining regularly after the surgery.
Main Outcome Measures: These included management of the technique, per- and post-operative complications, postoperative otoscopic findings (cholesteatoma recurrence, perforation, drainage, retractions) and hearing.
Results: No complication occurred during or after surgery. Palisade cartilage reconstruction technique took some additional time, however, it was not more than half an hour. As the number of patients was too small and follow-up time was too short, surgical and functional results were not discussed. However, there has been no recurrence, retractions and re-perforation up to now (mean follow-up time is six months).
Conclusions: The pathology in the anterior attic, tympanic sinus and posterior tympanum could be safely removed via Tos technique. Palisade cartilage technique could be useful for preventing retractions after tympanoplasty in cholesteatoma surgery. Finally, the combination of Tos and Heermann techniques might be a good choice for cholesteatoma treatment in selective cases. However, long-term results of a larger patient group should be analyzed.
Key words: Cholesteatoma; Treatment; Surgical technique; Complications; Tympanic membrane retraction.
Pro Otology 1: 22-25, 2002
The first and main goal in cholesteatoma surgery is to remove the disease and to prevent the occurrence of cholesteatoma. However, preservation or reconstruction of the hearing mechanism, and quality of life of the patient after surgery should also be considered in the treatment whenever possible. Cholesteatoma surgery should be individualized according to the prevailing pathoanatomy, as there is no method that is superior in all cases (1).
The classic combined-approach tympanoplasty, or the classic intact canal wall mastoidectomy, consists of a large mastoidectomy with an intact but thin bony ear canal wall, and a posterior atticotympanotomy (2). Removal of the cholesteatoma from the tympanic sinus and cleaning of the stapes through the posterior tympanotomy is difficult under narrow anatomic conditions; it can be complicated and sometimes impossible (1,3).
It is also difficult to remove cholesteatoma from the anterior attic through the mastoidectomy. These are the reasons why these regions are the most frequent places of residual cholesteatoma (4,5). In addition, postoperative attic retractions may result in development of recurrent cholesteatoma. So, most surgeons have gone back to canal wall down methods, whereas some prefer the intact canal wall technique with two stages. The reason for a second look is mainly to detect residual cholesteatoma in the attic and to repair attic retractions and remove recurrent cholesteatoma (3).
Tos modified combined-approach tympanoplasty in 1970, mainly to avoid second look operations and revisions, which usually end in a canal wall down procedure (6,7). The principle of this modified technique is to create such conditions in the attic that the retraction does not necessarily lead to recurrent cholesteatoma requiring re-operation, but most often to a peaceful, small cavity with an acceptably wide access (1).
In addition, modified combined-approach tympanoplasty (Tos technique; Fig. 1) has several advantages when compared with the classic combined-approach tympanoplasty (1,3,7). Removal of cholesteatoma from the tympanic sinus is safer and easier after drilling of the posterior wall of the bony annulus (otosclerosis drilling). All surgeons have extensive experience of operating on the stapes and footplate through this direct route. This can be the reason why the frequency of residual cholesteatoma in Tos technique (1,3,8-11) is considerably lower than that in classic combined-approach tympanoplasty (4,5) in the literature. Atticotomy provides an opportunity for a direct survey of the anterior attic, this being the second most frequent location of residual cholesteatoma (1,7).
The disadvantage of an atticotomy is that a new locus minoris resistentiae is created in epitympanum, where a retraction may occur. However, according to Tos' study, which consisted of the results of 133 patients, in cases with intact bridge, the retraction has appeared between the bridge and pars tensa but not at the site of atticotomy (1). Although retractions usually develop into self-cleansing cavities, unsafe retractions with insufficient cleaning, leading to retraction cholesteatoma may occur, even and more with bone reconstruction (7).
Heermann (12) claims that reconstruction of tympanic membrane and epitympanum with cartilage palisades has excellent results, because palisade cartilage technique, developed by Heermann et al (13), prevents twisting of cartilage, which is the case with large cartilage plates. More recently, Andersen et al (14) reported that palisade cartilage technique prevents efficiently postoperative retractions of the tympanic membrane after cholesteatoma surgery in children. Reconstruction of the attic and the tympanic membrane with cartilage palisades may also be effective against possible postoperative retractions in Tos technique, so Heermann technique may lead to add one more advantage to Tos technique.
STEPS OF THE SURGICAL TECHNIQUE
1. Transcanal and retroauricular incisions:
The operation begins endaurally through a speculum. A circumferential incision is performed starting anteriorly at the 3-o'clock position, continuing towards the 12-o'clock position, and then around to the 5-o'clock position. Then, using the sickle knife, a radial incision is made at the 5-o'clock and another at the 12-o'clock positions, starting at Shrapnell's membrane. The purpose of these incisions is to avoid tearing the ear canal skin during elevation.
After endaural incisions, operation is continued via retroauricular approach. A retroauricular incision, 1 cm behind the postauricular fold, is performed, going through the skin, subcutaneous tissue, and periosteum directly to the bone. The subcutaneous flap is elevated toward the suprameatal spine and the entrance of the bony meatus. The posterior part is elevated, exposing the cortical bone of the mastoid process. After placing self-retaining retractor, posterior half of the ear canal skin is elevated as for as circumferential incision, approximately 6 mm lateral to the annulus. The extent of the elevation of the ear canal skin depends on the cholesteatoma type. Elevation of the skin has to be extensive anteriorly in attic cholesteatoma, and inferiorly in tensa cholesteatoma (7).
2. Transcanal posterior tympanotomy:
The operation may be initiated by an intact canal wall mastoidectomy to assess the extent of cholesteatoma growth, but Dr. Tos prefers the order of steps, which is described in the present paper (3,8). The posterior tympanomeatal flap along with the fibrous annulus is elevated, and a large posterior tympanotomy is performed, exposing the posterior part of the tympanic cavity as well as the ossicular chain (7).
3. Drilling of the posterosuperior bony annulus (otosclerosis drilling):
An "otosclerosis drilling" of the posterior bony annulus is performed so that the entire tympanic sinus and footplate are visible (Fig. 1). So, all diseased material from the tympanic sinus and posterior tympanum can be removed more safely than through a transmastoid posterior tympanotomy (1,3).
4. Transmeatal atticotomy:
By continuous drilling of the ear canal along the tympanosquamous suture, a small plateau is created at the level of the lateral attic wall. The atticotomy opening is then drilled out and widened anteriorly and posteriorly, so that only a thin bony bridge is preserved (Figure 1). In the case of a large spontaneous bone erosion of the superior wall, this is widened, but the remaining bridge is preserved. The cholesteatoma from the attic could then be safely removed and especially the anterior mallear fold and anterior attic could be properly visualized (1,7). If preoperative Valsalva's maneuver is negative, bougienage of the Eustachian tube can be performed (7).
5. Transcortical intact canal wall mastoidectomy:
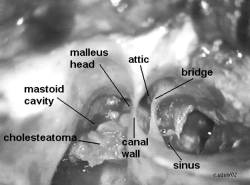
Cortical mastoidectomy with preservation of the intact wall, which must be carefully thinned, is always performed, leading careful and safely cleaning of the colesteatoma throgh three accesses; the cortical mastoidectomy, atticotomy, and tympanotomy (Fig. 1). In case of retraction, which often starts between the neck of malleus and the bridge, the latter will be surrounded by keratinized stratified epithelium and resorbed, just as the thin ear canal wall is slowly resorbed. Gradually, the access to the retraction is widened, cleaning becomes easier, and the retraction, which may first have been unstable, is often spontaneously transformed into an open cavity (1,3,7,8).
6. Reconstruction of the attic and the tympanic membrane:
The atticotomy opening can be covered either with fascia, cartilage, or a piece of cortical bone. Previously, Tos preferred to use fascia to cover atticotomy in order to detect through this opening any residual cholesteatoma (1,3,7). However, after finding good results in his research on palisade cartilage tympanoplasty in cholesteatoma cases (15), he prefers to use cartilage palisades for reconstruction of the tympanic membrane and the posterior canal defect as well as the atticotomy opening (Tos M. Personal communication, Copenhagen, April 2001 and Edirne, September 2001).
Intact ossicular chain should be preserved whenever possible. If it is not intact, ossiculoplasty is performed with autologous or homologous ossicles or cortical bone before palisade cartilage reconstruction (1,3).
The cartilage for palisade technique can be taken both from the concha and the tragus. The cartilage is then, cut by scalpel into thin (about 0.5 to 1 mm) slices, while preserving the perichondrium on one side of the cartilage. Palisades are placed over the attic, and over the bony annulus, parallel to the malleus handle, and beneath the fibrous annulus (Figure 2). Palisades must carefully cover posterior bony annulus and otosclerosis drilling, and then tympanomeatal and skin flaps, and fascia (if used) are replaced. To cover the palisades with fascia is not necessary for the ones used for tympanic membrane reconstruction. If ossiculoplasty is performed, palisades can be placed on to the ossicle or (shorter palisades) between the ossicle and the bony annulus (13,14).
A ventilation tube, 3 to 5 mm in diameter, is placed in the mastoidectomy cavity through a separate incision behind the skin incision and removed together with the ear canal pack, after three weeks. The ear canal is filled with Gelfoam balls to secure the ear canal skin flaps, as well as a 1-cm wide strip of gauze moistened with oxytetracycline and hydrocortisone ointment. If preoperative Valsalva's maneuver is negative, the patient performs a Valsalva's maneuver twice a day from the first week (7,8).
In their study on 273 patients with attic cholesteatoma, Lau and Tos (16), separated the patients into two groups with similar preoperative findings, and they followed the patients. One of these groups consisted of 161 ears, which were operated on Tos tecnique, and the mean follow-up was 8.25 (3-19) years. The other group consisted of 112 ears, which were operated on canal wall down mastoidectomy, and the mean follow-up was 10.75 (3-22) years. They have found that, recurrence (6.2-6.25) and reoperation (13-16 %) rates were almost the same in both techniques. Hearing in canal wall down group was slightly poorer than that in Tos technique group. Moreover, cavity problems and tympanic membrane pathologies were more common in canal wall down group.
Patients should be closely followed after closed techniques like Tos technique. When hearing detoriates, or persistent otorhea, residual or recurrent cholesteatoma is detected, re-operation is necessary. Tos technique can be employed with advantage in two-third of ears with attic cholesteatoma (2,16). The canal wall down technique is preferred in: (a) ears with slight or lacking pneumatization of the mastoid process; (b) ears with pronounced resorption of the posterior ear canal wall and lacking ossicles in the attic; (c) ears with severe middle ear pathology like cholesteatoma in the tubal orifice; or (d) ears requiring re-operation because of recurrent cholesteatoma (16).
Heermann's palisade cartilage technique has been shown to be useful for preventing retractions after tympanoplasty in cholesteatoma surgery (14,15). It has also been shown that 0,5 mm-thick cartilage palisades are similar to the tympanic membran in their acoustic properties. However, in chronic tubal dysfunction, like in cholesteatoma patients, or adhesive otitis, thicker palisades are advised to be used for preventing retractions (17). Tos (15) and Andersen et al (14) used about 1 mm thickness cartilage palisades for reconstruction of the tympanic membrane after one stage surgery for tensa cholesteatoma in children. They have found that postoperative hearing was good together with efficient prevention of postoperative retractions.
Between July 2001 and January 2002, I have performed Tos technique together with palisade cartilage reconstruction in three patients with cholesteatoma. No complication occurred during or after surgery. Palisade cartilage reconstruction technique took some additional time, however, it was not more than half an hour. As the number of patients is too small and the follow-up time is too short, surgical and functional results are not discussed in this paper. However, there has been no recurrence, retractions and re-perforation up to now (mean follow-up time is six months). Operation and postoperative eight-month endoscopic view of one of the patients are shown in Figures 1, 2 and 3, respectively.
In conclusion, the combination of Tos and Heermann techniques may be a good choice for cholesteatoma treatment in selective cases. However, long-term results of a larger patient group should be analyzed, and comparison with other techniques should be performed for an objective outcome.
ACKNOWLEDGEMENT
I thank Dr. Per Caye-Thomasen, from Gentofte University Hospital, Denmark, for sending me his accepted paper (14th reference).
REFERENCES
Tos M. Modification of combined-approach tympanoplasty in attic cholesteatoma. Arch Otolaryngol 1982;108:772-8.
Jansen C. Cartilage tympanoplasty. Laryngoscope 1963;73:1288-94.
Tos M. Modification of intact canal wall technique in the treatment of cholesteatoma. Adv Otorhinolaryngol 1987;37:104-7.
Glasscock ME, Miller GW. Intact canal wall tympanoplasty in the management of cholesteatoma. Laryngoscope 1976;86:1639-57.
Smyth GD. Postoperative cholesteatoma in combined approach tympanoplasty. Fifteen year report on tympanoplasty. Part I. J Laryngol Otol 1976;90:597-621.
Tos M. [Operative therapy for chronic otitis media and middle ear cholesteatoma with preservation of the posterior auditory canal wall ("intact wall technique") (author's transl)] HNO 1978;26:217-23.
Tos M. Manual of middle ear surgery. Vol 2: Mastoid surgery and reconstructive procedures. Stuttgart: Thime, 1995.
Tos M, Lau T. Attic cholesteatoma. Recurrence rate related to observation time. Am J Otol 1988;9:456-64.
Lau T, Tos M. Treatment of sinus cholesteatoma. Long-term results and recurrence rate. Arch Otolaryngol Head Neck Surg 1988;114:1428-34.
Lau T, Tos M. Tensa retraction cholesteatoma: treatment and long-term results. J Laryngol Otol 1989;103:149-57.
Tos M, Lau T. Late results of surgery in different cholesteatoma types. ORL 1989;51:33-49.
Heermann J. Auricular cartilage palisade tympano-,epitympano-, antrum- and mastoid plasties. Clin Otolaryngol 1978;3:443-6.
Heermann H, Heermann J, Kopstein E. Fascia and cartilage palisade tympanoplasty: nine years?experience. Arch Otolaryngol 1970;91:228-41.
Andersen J, Caye-Thomasen P, Tos M. Cartilage palisade tympanoplasty in sinus and tensa retraction cholesteatoma. Otol Neurotol 2002 (in press).
Tos M, Andersen J, Caye-Thomasen P. Palisade cartilage technique to prevent retraction after one-stage surgery for sinus- and tensa-retraction cholesteatoma in children. Proceedings of the 4th Extraordinary International Symposium on Recent Advances in Otitis Media, 16-20 April 2001, Sendai, Japan 2002 (in press).
Lau T, Tos M. Attic cholesteatoma: Comparison between canal wall up and canal wall down technique. In: Tos M, Thomsen J, Peitersen E, eds. Cholesteatoma and mastoid surgery. Amsterdam: Kugler, 1989:961-6.
Zahnert T, Huttenbrink KB, Murbe D, Bornitz M. Experimental investigations of the use of cartilage in tympanic membrane reconstruction. Am J Otol 2000;21:322-8.
|
Pro Otology |
Journal Home Contents Preview Next |