|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 2, No 2:69-72 © 2002
All rights reserved. Published by Pro Otology Association
Hearing Loss in Some Metabolic Bone Diseases
Radost Hristova
Clinic of Otorhinolaryngology, Medical Faculty, Trakia University, Stara Zagora
ABSTRACT
Objective: To overview the published data devoted to the hearing loss in some metabolic bone diseases and to underline the need of more detail and complete investigations for clarifying the mechanisms of hearing loss in diseases such as Osteogenesis Imperfecta, Paget's disease and osteoporosis.
Data Sources: Sources used were relevant clinical and basic science publications from 1960 to 2001.
Study selection: The selected articles include information about the involvement of the temporal bone and hearing loss in patients with a metabolic bone disease.
Conclusions: The pathological changes in metabolic bone diseases may involve any bone of the skeleton including the bones of the ossicular chain, the bony cochlear capsule and the bony canals of the ear. The changes in bone mineral content or density reflect a change in sound transmission and a hearing loss might be determined in patients suffering from such diseases.
Key Words: Hearing loss, Paget's disease, Osteoporosis, Osteogenesis imperfecta.
Pro Otology 2: 69-72, 2002
INTRODUCTION
Bone turnover and remodeling occurs throughout life and involves the two-coupled processes of bone formation by osteoblasts and bone osteocytes. The metabolic bone diseases may reflect disturbances in the organic matrix, the mineral phase, and the cellular processes of remodeling, which regulate skeletal mineral homeostasis. These disorders may be hereditary or acquired and usually affect the entire bony skeleton.
Since these diseases primarily affect bone, pathological changes might be expected in the bones of the ossicular chain, the interface between the stapes and the oval window, the bony cochlear capsule, and the bony canals by which the nerve fibers leave the ear and enter the internal auditory canal. This also suggests the possibility the generalized metabolic bone disorders to be the underlying cause in some cases of otosclerosis (1,2). If normal transmission of sound were a function of the total amount of bone present in the ossicular chain, it would be logical to expect decreased sound transmission in metabolic bone diseases such as Paget's disease of bone, osteogenesis imperfecta and osteoporosis. In fact such changes in the hearing levels have been explored in details from many authors (5,9,11,16,17,20,30,33,36,38) in patients with Paget's disease and osteogenesis imperfecta. The hearing loss in osteoporosis is not still well defined.
PAGET'S DISEASE OF BONE
In 1876 Sir James Paget (3) described for the first time a chronic bone disorder, characterized by spreading osteolytic and osteoblastic changes affecting mainly the pelvis, lumbosacral spine, skull, femoral and tibial bones. He called the condition "osteitis deformans". The etiology of Paget's disease remains controversial (4,5). None of the several hypotheses proposed has yet met with a consensus.
In this disorder the general organization of the affected bone is completely disorganized. Structural disturbances are found in dense cortical bone as well as in spongy trabecular bone and the morphological distinction between them is lost (6). Any bone may be affected by these changes. The temporal bone is involved in perhaps 50% of the cases with clinical manifestations (6,7).
The relation between bone pathology of the skull and hearing loss has been investigated primarily through studies of persons with Paget's disease of the bone and cochlear otosclerosis (7-9). In Paget's disease the haversian bone of pars petrosa is affected first, and because of the demineralization of this bone, the cochlear capsule and the ossicles become more prominent than usual. The progression of the involvement follows a path from the apex to the base of the petrous pyramid. The internal auditory canal is involved first, followed by the cochlea and the vestibular system. Degenerative changes occur in the stria vascularis with atrophy of the structures of the cochlear duct and vestibular labyrinth. Both secondary endolymphatic hydrops of the cochlear duct and saccule, and atrophy of the membranous semicircular canals have been described (6).
Deafness (sensorineural, conductive or mixed), is a very common complication of Paget's disease, occurring in about 30-50% of the patients with pagetic lesions of the skull (5,6,10,11) and is usually fairly symmetrical (6). It may appear early in the course of the disorder and may sometimes lead to the discovery of Paget's disease (12). It has been concluded that the hearing losses in Paget's disease are caused by changes in bone density, mass and form that serve to dampen the finely tuned motion mechanics of the middle and inner ears (13).
According to some studies (6) the causation of the conductive component of deafness is the involvement of the ossicles, mainly the malleus head by osteitis deformans. The footplate is immune from involvement in Paget's disease, though the remainder of the ossicular chain is affected (14). As the Paget's disease can be symptomless apart from the otological features, the patients with a large element of conductive deafness could be considered to have otosclerosis
The histopathological changes in the temporal bone also have a resemblance to otosclerosis (6,14-16).
The outstanding difference between the two lesions being the tendency of the former to originate from a sharply limited region of the temporal bone, while Paget's disease, although frequently affecting the temporal bone, involves the whole otic capsule from around its periphery.
Some authors (7-9) found that demineralization of the cochlea and otic capsule was associated with sensorineural hearing loss and that the degree of cochlear demineralization corresponded directly to the severity of the hearing loss. Secondary neuronal degeneration seems likely in the later stages of the disease, and if there is sufficient softening and deformity of the skull base the nerves may even be involved in the internal auditory meatus. Some findings support the principle that hearing loss in Paget's disease of bone is generally associated with intact auditory nerve function (17).
OSTEOGENESIS IMPERFECTA
Osteogenesis imperfecta, known also as fragilitas osseum or the syndrome of Van der Hoeve and De Kleyn is a relatively rare disease. It belongs to a group of hereditary disorders of collagen, with a dominant mode of inheritance, incomplete manifestation, and varying degrees of expressivity from family to family. It's resulting from mutations in genes that encode Type 1 collagen, the major structural protein in the body (18). Several molecular defects have been found in persons with different types of osteogenesis imperfecta (19). According to the contemporary classifications of the disease (20) there are four types of osteogenesis imperfecta the classic triad of Van der Hoeve and de Kleyn (blue scleras, fragile bones and deafness) is manifested in Type I and III.
Bone samples from patients with the severe congenital form of osteogenesis imperfecta are characterized by the absence of an organized trabecular pattern. The osteocytes are crowded within the bone, reflecting the diminished collagen synthesis by the crowded osteoblasts at the surface (21). In the less severely affected individuals, the bone is generally lamellar in pattern though even in this bone the osteocytes are generally crowded and the lamellae may be observed to be thinner than those seen in age matched control subjects.
The first association of osteogenesis imperfecta with hearing loss is made in 1912 from Adair-Dighton but one of the largest recent studies of osteogenesis imperfecta is that of Smars (22). The clinical features from his data shows that deafness was encountered in 22,6 % of surviving cases and that there was no relationship between hearing loss and the severity of the disease. Differences were shown between patients with different clinical types of osteogenesis imperfecta as delineated in the Sillence classification; hearing loss was significantly less common in the type IV disease than in the type I disorder (23). Deafness was equally common among sporadic and familial cases.
Because of the superficial resemblance of the deafness in osteogenesis to the deafness of otosclerosis there has been a natural tendency for otologists to consider them as different manifestations of the same disease. Shea and Postma (24) claimed that osteogenesis imperfecta differs from otosclerosis in the following ways: earlier onset, more severe middle ear involvement, and a highe incidence of sensorineural hearing loss.
Studies by Pedersen (25) have shown significant differences in the microscopic pathology of the stapes footplate in otosclerosis and in osteogenesis imperfecta. He concluded that microscopic fractures of the footplate and subsequent healing are the important causes of the stapediovestibular fixation in osteogenesis imperfecta. Precechtel (26) also considered the differences between these two diseases based on histological and histochemical evidences.
The hearing loss in the van der Hoeve syndrome may start in childhood or be delayed well into adult life. It usually progresses from the third decade and is most commonly conductive but also can be sensorineural or mixed (18).
The conductive or mixed deafness may be the result of a deficient crural arch, stapes fixation by a focus of otosclerosis, or both (27,32,35). Opheim (28) seems to have been the first to observe degeneration of the stapedial crura. Others including Patterson and Stone (29) have noted similar changes. Healed fractures of the handle of the malleus were also seen. Except all these changes structural defects are suggested to exist in the whole ossicular chain (27,30).
Otosclerosis occurring in association with osteogenesis imperfecta appears to have a more aggressive behavior, often leading to total obliteration of both windows and sensorineural deafness. This degree of pathology compromises the success of stapes surgery (31). In such cases the amplification is often discussed alternative (32).
OSTEOPOROSIS
Osteoporosis is a frequent condition and may coexist with other primary bone disorders. Various definitions have been offered to describe the outcome of events (fragility fractures), the process giving rise to porous bones, or the resultant diminution in bone mass. The following definition is now generally accepted: "A progressive systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture" (33).
|
||||||
Osteoporosis could be primary (postmenopausal, senile, idiopathic and juvenile) or secondary. More than 95% of adults with osteoporosis have involutional osteoporosis - Type I (postmenopausal) and Type II (senile), the causes of which are uncertain. An indirect association may be mediated through postmenopausal estrogen use, vitamin D nutriture and other factors that covary with age such as illness and medication use.
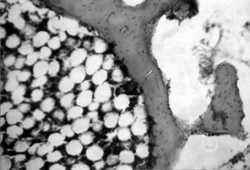
Histologically, the amount of cortical and cancellous bone in osteoporosis is decreased compared to the normal for a similar site, sex, and age. The bone that remains has a lamellar structure and osteoid seams of normal width. The bone cortices are thinned, and the haversian canals are widened. The trabeculae of cancellous bone are decreased in size and number. They are thin, discontinuous, and widely separated (Fig. 1, 2). The rate of bone resorption exceeds the rate of bone formation (6).
In 1994 the WHO proposed guidelines for the diagnosis of osteoporosis based on measurement of bone mineral density (39). The method is called densitometry and is used for studying the state of bone mass in generalized bone diseases. In patients with primary osteoporosis it gives some evidence that osteoporosis does not spare the bones of the skull (35-37). A direct association between bone mass and hearing loss assumes that measured bone mass of the femoral neck reflects bone mass of the petrous temporal bone (including the cochlea and otic capsule). That demineralization has been related to hearing loss in other metabolic bone diseases (7-9).
Henkin et al. (38) found some correlation between roentgenographically demonstrable pathology and audiometric findings in some patients with osteoporosis. However, the severity of the hearing losses cannot be consistently correlated with the degree of roentgenographically demonstrable changes. This situation is also observed in patients with otosclerosis with these and other pathological changes (39-41). Similarly, there does not appear to be any correlation between duration and severity of metabolic bone disease and hearing loss (38). The pure-tone audiometry is the most reliable method for clarifying the type of hearing loss (43) (Fig. 3).
All these findings raise the question of the relationship of senile osteoporosis to that variant of presbyacusis described by Schuknecht (14) in which there is spiral ligament atrophy similar to that seen adjacent to areas of otosclerosis or Paget's disease of bone.
CONCLUSIONS
The temporal bone doesn't remains isolated from the general metabolic changes in the skeleton. Probably it has typical features of exchange except its anatomical ones.
The bone of the cochlear caps ule is lamellar bone with few haversian canals and vascular elements, and thus consists of maximally compact bone tissue (42). Thus, bone lysis by metabolic bone diseases would result in density values less than normal, whereas bone sclerosis could only thicken the cochlear capsule, not increase its mineral density.
The finding in this review support the presence of a general mechanism causing hearing loss in Paget's disease of bone and osteogenesis imperfecta but are still not well defined in osteoporosis. In cochlear capsules affected by osteoporosis, leakage or distortion of sound energy conceivably may be due to a widespread defect in the surrounding bone.
Further studies are needed to elucidate this mechanism, and knowledge of such phenomena as the relationships demonstrated here would be important to this work.
REFERENSES
Soifeer N, Altman F, Endahl GL et al: Biochemical studies of otosclerosis. Enzymes and protein in malleus and incus. Acta Otolaryngolol 1967;63:587-94.
Mauerer H. Biochemical aspects of otosclerosis. Arch Otolaryngol 1967;85:238-42.
Paget J. On a form of Chronic Inflammatiion of bones. Medico-Chirrurgical Trans (London) 1877;60:37-63.
Basle MF, Rebel A, Audran M. Paget's disease of bone. The metabolic and molecular basis of aquired disease. London, Norfolk: Paston Press 1990;1783-97.
Singer FR, Mills BG. The etiology of Paget's disease of bone. Chin Orthop 1977;127:37-42.
Davies DG: The temporal bone in Paget's disease. J Laryngol Otol 1970;84(6):553-60.
Pestasnicyk J. Tomography of the temporal bone in Paget's disease. Am J of Roengenology, Rradium Therapy & Nuclear Medicine 1969;105:838-43.
Huizing E, De Groot J. Densitometry of the cochlear capsule and correlation between bone density loss and bone conduction hearing loss in otosclerosis. Acta Otolaryngol (Stockh) 1987;103:464-8.
9. De Groot J, Huizing E, Damsma H et al. Labyrinthine otosclerosis studied by means of a new computed tomography technique. Ann Otol 1984;94:223-7.Menzies MA, Greenberg PB, Joplin GF. Otological studies in patients with deafness due to Paget's disease before and after treatment with synthetic human calcitonin. Acta Otolaringol 1976;79:378-83.
Sparrow NL, Duvall AJ III. Hearing loss and Paget's disease. J Laryng Otol 1967;81:601-11.
Chakravorty NK. Neurological complication of Paget's disease of bone. Br J Clin Prac 1985;39:335-8.
Khetarpal U, Schuknecht HF. In search of pathologic correlates for hearing loss and vertigo in Raget's disease. A clinical and histopathologic study of 26 temporal bones. Ann Otol Rhinol Laryngol Suppl 1990;145:1-16.
Schuknecht HF. Pathology of the ear. Medical Journal Harvard 1974;49:1256-7.
Ruedi L. Are there cochlear shunts in Paget’s disease and Recklinghauses’s Disease? Acta Otolaryngol 1968;65:13-24.
Lindsay J and Lehman R. Histopathology of the temporal bone in advanced Paget’s disease. Laryngoscope 1969;79(2):213-27.
Monsell EM, Cody DD et al. Hearing loss in Paget's disease of bone: the relationship between pure-tone thresholds and mineral density of the cochlear capsule. Hear Res 1995;83:114-20.
18 Richard JH, Smith and Simon IA. Hereditary hearing impairment. Otorhinolaryngology, Head and Neck Surgery 1996;15:1075-86.
Byers PH, Steiner RD. Osteogenesis Imperfecta. Ann Rev Med 1992;43:269-70.
Sillence DO. Osteogenesis imperfecta: An expanding panorama of variants. Clin Orthop Res 1981;159:11-25.
Bullough PG. Nonneoplastic Disease of Bones. Diagnostic Surgical Pathology, Raven Press, 1992;496:4-10.
Smars G. Osteogenesis imperfecta in Sweden. Stockholm: Scandinavian University Press, 1961.
Paterson CR, Monk EA et al. How common is hearing impairment in osteogenesis imperfecta. J Laryngol Otol 2001;115:280-2.
Shea JJ and Postma DS. Findings and long-term surgical results in the hearing loss of osteogenesis imperfecta. Arch Otolaryngol 1982;108(8):467-70.
Pedersen U. Osteogenesis imperfecta clinical features, hearing loss and stapedectomy. Biochemical, osteodensitometric, corneometric and histological aspects in comparison with otosclerosis. Acta Otolaryngol Suppl 1985;415:1-36.
Precechtel A. Ontogenic aspects of hearing disorders in otosclerosis as a disease and as a sign of osteogenesis imperfecta with Van der Hoeve-de Klein syndrome. Cesk Otolaryngol 1965;14(5):261-7.
Pedersen U. Hearing loss in patients with osteogenesis imperfecta. A clinical and audiological study of 201 patients. Scand Audiol 1984;15(2):67-74.
Opheim O. Loss of hearing following the syndrome of Van der Hoeve-de Kleyn. Acta Otolaryngol 1968;65(3):337-44.
Patterson C and Stone H. Stapedectomy in Van der Hoeve’s syndrome. Laryngoscope 1970;80(4):544-58.
Shapiro JR, Pikus A et al. Hearing and middle ear function in osteogenesis imperfecta. Jama 1982;47:2120-6.
Garrentson TJ, Cremers CW. Stapes surgery in osteogenesis imperfecta: analysis of postoperative hearing loss. Ann Otol Rhinol Laryngol 1991;100-20.
Riedner ED, Levin LS et al. Hearing patterns in dominant osteogenesis imperfecta. Arch Otolaryngol 1980;106:737-40.
Consensus development conference. Diagnosis, prophylaxis and treatment of osteoporosis. Am J Med 1991;90:170-210.
Kanis JA, Gluer CC. An update on the diagnosis and assessment of osteoporosis with densitometry. Osteop Int 2000;11:192-202.
Clark K, Sowers MR et al. Hearing loss and bone mass. AEP 1995;5:8-14.
Mennier P, Bianchi G, Edouard C et al. Bony manifestations of thyrotoxicosis. Orthop Clin Norht Am 1972;3:745-71.
Khan A, Lore J. Osteoporosis relative to head and neck. J Med 1984;279-84.
Henkin RI, Lifschitz MD, Larson AL. Hearing loss in patients with osteoporosis and Paget's disease of bone. Am J Med 1972;263:383-92.
Rockert H, Engstrom H, Hallen O et al. Otosclerosis studied with x-ray microscopy and fluorescence microscopy after administration of tetracycline. J Laryngol & Otol 1965;79:305-13.
Carhart RC. Audiometric configurations in preclinical otosclerosis. Ann Otology & Rhinology 1967;68:769-814.
Kelemen G, Linthicum FH. Labyrinthine otosclerosis. Acta Otolaryng (Suppl) 1969;253.
Sorensen MS et al. Quantum type bone remodeling in the human otic capsule, morphometric findings. Acta Otolaryngol (Stockh), Suppl 1992;496:4-10.
Dimov. P. Chronic Otitis Media with Effusion. Stara Zagora: Ariel, 1997.
|
Pro Otology |
Journal Home Contents Preview Next |