|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 3, No 23:7785 © 2003
All rights reserved. Published by Pro Otology Association
CO2 Laser Stapedotomy in Primary and Revision Cases
S. Jovanovic, U. Schönfeld, H. Scherer
Ear, Nose and Throat Department, University Medical Center Benjamin Franklin,
Freie Universitat Berlin, Berlin, Germany
ABSTRACT
Objective: The idea of applying the CO2 laser as a precise and contact-free instrument in middle-ear surgery and especially in stapes surgery is based on the desire to reduce the complication rate of these interventions by further optimizing the surgical techniques. Today, using high-precision micromanipulators, the laser beam can be focused to a spot diameter of 180 µm. New application modes combined with scanner systems enable an exact adjustment to the demands of stapes surgery, thus permitting the finest microsurgical work.
Study design: Investigation of patients under CO2 Laser Stapedotomy.
Settings: Ear, Nose and Throat Department, University Medical Center Benjamin Franklin, Freie Universitat Berlin, Berlin, Germany.
Patiens: Primary and Revision Cases of Otosclerosis.
Conclusions: The risk of chain luxation, particularly footplate mobilization (floating footplate) or damage to the adjacent middle and inner ear structures is practically impossible with the limitation of the energy parameters used here.
One shot stapedotomy can be achieved by microprocessor-controlled movement of the focused laser beam over a defined area (diameter: 0.5 to 0.7 mm) by rotating mirrors. On the basis of experimental data, effective and safe parameters were determined with the CO2 laser and applied in the clinical routine. Compared to conventional techniques the CO2 laser irradiation enables precise and contact-free procedures on middle ear structures.
Key words: Stapedotomy, Otosclerosis, Middle ear surgery, Scanner systems.
Pro Otology 2-3: 77-85, 2003
Introduction
Although stapedotomy is a preferred operation in stapes surgery, mechanical instruments such as a drill or a perforator cannot create a precise, round perforation. In fact, in some situations, mechanical instruments can prove hazardous. For example, a partially fixed stapes is often accidentally mobilised by manipulations (floating footplate) and a thin footplate is not infrequently fractured. In obliterative otosclerosis, perforation of a thick obliterating footplate with the drill can result in significant inner ear trauma due to vibrations.
The aim of stapedotomy with the laser is to enable management of the stapes in such a way as to ensure the greatest possible protection of the inner ear and the avoidance of damage to residual middle ear structures. Advocates of the laser technique agree that noncontact laser vaporization of the bone covering the vestibule is less traumatic for the inner ear than manual instrumental extraction or perforation of the stapes footplate.
In 1980, Perkins and DiBartolomeo and Ellis used the argon laser for the first time, and in 1989 following the development of precision micromanipulators Lesinski successfully used the CO2 laser in stapes surgery (10,49,68). Nevertheless, their effectiveness and safety have been discussed still controversial (2,10,13-15,17,19,22,24-47,49-54,56-58,66,67,70,75,76,79,80,83-91,93). This initially led to skepticism regarding their application in stapes surgery.
Since the publication of the authors experimental and clinical studies confirming that CO2 laser is suitable for stapedotomy, this wavelength in the far infrared range has found greater acceptance and broader application in ear surgery (26-47). Particularly for revision stapedotomies but also for primary surgeries, clinical studies demonstrate that the CO2 laser achieves significantly better hearing results and less complication rates than conventional surgery (3,19,38,42,43,49-53,76).
The argon and KTP laser seem to prove their value in primary and revision cases, too (24,57,64,68,74,88,93). Here, the introduction of a fiberoptical micro-handpiece (Endo-Otoprobe), which in comparison with laser application by help of micromanipulators attached to the microscope has the advantage that due to the strong laser beam divergence at the exit of the optical fibre a rapid decrease of energy density in relation to the increase of distance will result (6,18,24). Thus, the penetration depth and temperature problem in the perilymphe with possible damage to the inner ear will be reduced. Moreover, the use of the fiberoptical microhandpiece facilitates the vaporization especially also of the anterior crus, while reducing the needed technical equipment (21). Nevertheless, the suitability of the argon and KTP laser for stapedotomy is doubtful in view of the lower absorption coefficient of the stapes for the argon and KTP beam and the considerable influence which the degree of pigmentation of the irradiated medium exerts on its effect with the resultant poor reproducibility of the perforation. The beam of the CO2 laser is far better absorbed at the footplate than that of the argon and KTP laser. This results in higher effectiveness, lower thermic side effects and better reproducibility of the perforation diameter (41).
From among the group of pulsed laser systems the Er:YAG laser at first seemed to possess the most suitable wave length for middle ear surgery. Due to different wave lengths and the differing relation of irradiation and time the impact and effectiveness of the Er:YAG laser as against the CO2 laser differ in the tissue. While the continuously radiating CO2 laser is suitable for use on soft tissue as well as if well focused for vaporization of thin bone structures the Er:YAG laser offers advantages mainly in the treatment of bone structures (8,20,23,34,35,39,41,44,62,63,65,71-73,77). However, as soon as bleeding occurs the oligothermic Er:YAG laser radiation is completely absorbed by blood and does no longer reach the intended area. It is then ineffective.
Moreover, the measured sound level in Er:YAG laser therapy is higher and implies the risk of inner ear trauma and tinnitus (20,37,39,47,73). Meanwhile it is suspected that the pressure waves resulting from Er:YAG laser therapy may cause transitory or even permanent inner ear damage such as deteriorated hearing of high frequencies or tinnitus (4,20 and own experiences). Thus, application safety in Er:YAG laser is less than in CO2 laser. For the time being the erbium laser may therefore not be recommended for stapes surgery.
Material AnD Methods
CO2 Laser and Application Systems
One of the great advantages of the CO2 laser for stapedotomy is its high absorption of radiation in the perilymph with a resultant low penetration depth of only 0.01 mm. The CO2 laser beam, which could not be adequately focussed in the past due to the longer wavelength and the poor beam quality, can now be focussed with high-precision micromanipulators to a spot diameter of about 180 µm at a focal length of 250 mm. Thus, values are reached which permit finest microsurgical work.
When applying laser irradiation with microprocessor-controlled rotating mirrors, the so-called scanner systems (SurgiTouch, Lumenis Co., modified according to authors recommendations), a spiral figure is traced within the defined pulse duration. This enables the CO2 laser to achieve a high power density with minimal side effects, even in large irradiation fields. At a working distance of 250 mm, the scanner can be set for irradiation fields of various sizes depending on the anatomical variations and pre-selected perforation diameter. Irradiation fields of 0.5 mm, 0.6 mm and 0.7 mm are suitable for stapedotomy. A radius of less than 0.5 mm or greater than 0.7 mm can be achieved with SurgiTouch, but is rarely applied. Thus, a suitable selection of laser parameters basically enables a single-shot footplate perforation of pre-selected diameter. The laser beam is guided via a hinged mirror arm to a micromanipulator connected to the operating microscope and transmitted from there into the operating area. 250 mm proved to be the most favourable working distance.Effective and Safe Laser Energy Parameters
Based on data obtained in petrous bone preparations, in a cochlea model (41) and in animal experiments earlier published, effective and save parameters for stapedotomy with the CO2 laser {Type 40C SurgiTouch (Lumenis Co.) and micromanipulators Acuspot 712 (Lumenis Co.)} were determined (Table 1 and 2) (46). The mode is continuous wave. A favourable pulse duration proved to be the shortest time of 0.03 s to 0.05 s. The choice of powers ranged from 1 W to 22 W (4000 - 88000 W/cm2). To reduce the thermic effects of CO2 laser irradiation, perforation of the footplate is performed by several juxtapositioned single shots with low power, a short pulse duration and a small beam diameter or by a microprocessor-controlled rotating laser beam with scanning figures of different irradiation diameters (SurgiTouch, Lumenis Co.).
CO2 laser irradiation of high power density and low single pulse energy is applied in this connection. Footplate perforations of defined diameter (0.5 - 0.7 mm) can usually be achieved by a single laser shot with rotating mirrors. If necessary, the perforation diameter can be increased by additional single shots without the rotating beam. Applying a good beam profile enables optimal tissue results with minimal thermic side effects. Restricting the laser energy parameters accordingly obviates any risk to middle and inner ear structures by thermic or acoustic stress.
|
|
Surgical Technique
A) Primary Surgery
Injection of 1% xylocaine with 1:200 000 epinephrine and preparation of the tympanomeatal flap are followed by the opening of the middle ear and the removal of the meatus bone covering the oval niche with the sharp double-end curette according to House or with the diamond drill while preserving the chorda tympani. As with the conventional technique, access to the oval niche is adequate when the pyramidal process and part of the tympanic segment of the facial nerve are clearly visible. Application of the CO2 laser is preceded by some test shots at, for instance, a wooden spatula in order to exclude a possible disadjustment between the HeNe pilot beam and the invisible far-infrared CO2 laser beam. If the pilot beam is not in conformity with the surgical beam, a correction can be effected prior to lasering. Ablation of the suprastructures and perforation of the footplate is then performed in a non-contact manner with the CO2 laser beam.
Vaporisation of the Stapedius Tendon
The stapedius tendon is first vaporised with 2 to 3 single pulses at low power of 2 W (power density 8000 W/cm2) and a pulse duration of 0.05 s. The developing smoke is removed by suction. In case of a favourable anatomical situation the stapedius tendon can be preserved.
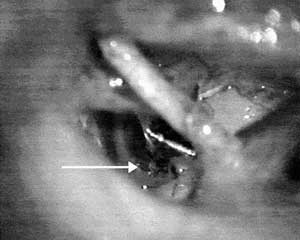
Separation of the Incudo-Stapedial Joint
The incudostapedial joint is then separated by vaporising the head of the stapes applying 8 to 14 single pulses of the laser beam at 6 W (power density 24000 W/cm2) and a pulse duration of 0.05 s (FIG. 1). The fact that CO2 laser beam does not fall in entirely perpendicular to the joint necessitates additional instrument-assisted checking and, if necessary, severing of residual connections between the processus lenticularis and the caput stapedis.
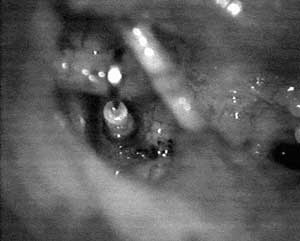
Vaporisation of the Posterior Crus
The posterior crus of the stapes is severed near the footplate with 4-8 pulses and the same power of 6 W (power density 24000 W/cm2) and pulse duration of 0.05 s applied for the incudostapedial joint (FIG. 2).
While severing the joint and the posterior crus with this relatively high laser power, care must be taken that middle ear structures situated in the beam direction (footplate, facial nerve canal, etc.) are not irradiated by mistake and damaged. Reliable protection is provided by filling the cavum tympani with saline or covering of these structures with saline tinctured gelatin sponge (Gelita, Spongostan, etc.).
Vaporisation of the Anterior Crus
The anterior crus of the stapes is often not directly accessible to the laser beam; it is possible with the aid of a mirror to deflect the CO2 laser beam in such a way as to enable vaporisation of the anterior crus under visual control. The mirrors available to us so far have not yet been optimal in this respect, so that we have preferred in most cases to fracture the anterior crus conventionally with the hook.
If it is partially visible, it is likewise vaporised with the CO2 laser beam using the same parameters applied for the posterior crus. Even in cases of incomplete severance, it can thus be submitted to controlled fracturing with the hook at the vaporised site. Footplate mobilisation or even partial or total footplate extraction is thus almost entirely excluded.
Perforation of the Footplate
Vaporisation of the posterior part of the footplate can be performed after the suprastructure has been removed. The aim is to achieve an adequately large, nearly round, reproducible perforation of 0.5 mm to 0.7 mm with one shot application or with a few juxtapositioned, slightly overlapping multiple applications.
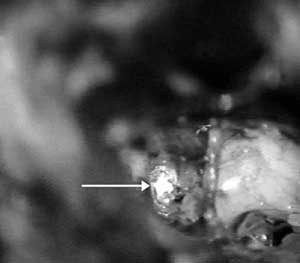
One shot Application Technique
When applying laser irradiation with a scanner system (SurgiTouch, Lumenis Co., modified according to our recommendations), a spiral figure is traced within the defined pulse duration. This enables the CO2 laser to achieve high power densities and thus optimal results with minimal side effects even in large irradiation fields. At a working distance of 250 mm, the scanners can be set for irradiation fields of various sizes depending on the anatomic conditions and defined perforation diameter. Irradiation fields of 0.5 mm, 0.6 mm and 0.7 mm are suitable for stapedotomy. A radius of less than 0.5 mm (0.4 and 0.3 mm) or greater than 0.7 mm (0.8, 0.9 and 1 mm) can be achieved with SurgiTouch but is rarely applied. Thus, a suitable selection of laser parameters basically enables a single-shot footplate perforation of defined diameter. The selected powers for the one shot application technique with rotating mirrors (SurgiTouch, Lumenis Co.) are 20 W to 22 W (power density 80,000-88,000 W/cm2). The pulse duration involved ranges between 0.03 and 0.05 s per pulse. Depending on the thickness of the footplate and the irradiation diameter of the scanning figure applied, the perforation diameters with the one shot stapedotomy technique with rotating mirrors range between 0.5 and 0.7 mm, in 90 % of the cases (FIG. 3). In those cases in which the desired perforation diameter is not achievable with one shot the enlargement of the perforation is performed by additional laser applications without the scanner system.
Mulitple shot Application Technique
When a scanner system is not available the stapedotomy can be performed with several juxtapositioned laser applications of the focussed laser beam (beam diameter 180 µm) in a circular manner. The selected power for the multiple shot application technique is 6 W (power density 24000 W/cm2) and the pulse duration 0.05 s. The number of pulses varies between 6 and 12 applications depending on the thickness of the footplate. During the enlargement of the perforation with additional laser shots until the desired perforation diameter of 0.5 - 0.7 mm is achieved, care must be taken that the vestibulum is filled with perilymph to ensure adequate protection of inner ear structures and prevent damages by direct laser irradiation. If the perilymph is inadvertently aspirated from the vestibulum no further laser irradiation must be applied to the footplate.
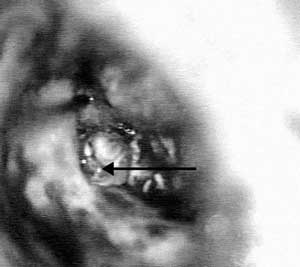
A platinum teflon piston of 0.4 mm respectively 0.6 mm in diameter is then inserted in the perforation and fixed to the incus neck. Finally, the oval niche is sealed with connective tissue or a blood clot (FIG. 4).
B) Special Cases
Obliterative OtosclerosisUsing the drill to perforate a thick footplate obliterating the oval niche can cause a significant inner ear trauma through vibrations. CO2 laser stapedotomy, on the other hand enables the ear surgeon to vaporise a perforation in the stapes footplate regardless of its thickness or degree of fixation without mechanically traumatising the inner ear.
After removal of the suprastructure, the otosclerotic foci obliterating the oval niche are extensively and symmetrically ablated by applying the laser irradiation with the SurgiTouch (power 20-22 W, pulse duration 0.03 to 0.05 s, scanner diameter 0.5 to 0.7 mm) until the lateral borders of the oval window can be precisely identified. In part lower powers are applied around the oval niche to avoid inadvertently opening the inner ear. Ablation of these bone masses yields large amounts of thermic products such as carbonisation and crystallisation (FIG. 5). Since the crystallisation product leads to increased reflection of the CO2 laser irradiation and thus to ineffectiveness and lower ablation, it must be removed with conventional instruments such as a curved needle or suction device. The vestibulum is opened at the centre of the oval niche. The perforation is then concentrically enlarged to the desired diameter by further single applications. The prosthesis is inserted in the typical manner.
Floating Footplate
Particularly with a partially fixed stapes, manipulation by conventional stapedotomy often leads to accidental mobilisation of the stapes and results in a so-called floating footplate. The operation is usually abandoned or total stapedectomy carried out, since the footplate can no longer be perforated with conventional instruments in many such cases. On the other hand, the CO2 laser achieves a noncontact perforation of defined diameter even in a floating footplate without the associated trauma caused by conventional instruments. A platinum teflon piston can then be inserted in such a perforation. However, the incidence of a floating footplate is extremely low in laser stapedotomy compared to conventional operations. In authors experience it is as low as 0.5%. A stapedectomy was not necessary in any of the cases.
|
|
Revision Surgery
Successful restoration of hearing in revision stapedotomies comprises the precise identification and correction of the particular abnormality without damaging the inner ear.
Following the elevation of the tympanomeatal flap, the middle ear is first inspected. The integrity and mobility of the malleus and incus are checked by palpation with the Rosen needle.
With the experimentally determined effective and safe laser energy parameters the frequently existing adhesions are first vaporised with the CO2 laser. Using a beam diameter of 0.18 mm, low powers of 1 to 2 W at a pulse duration of 0.05 s are adequate for this purpose. If the SurgiTouch scanner system is used, powers of 4 to 8 W at a pulse duration of 0.03 to 0.05 s and variable scanner diameters (0.3 to 0.5 mm) are sufficient for the soft tissue treatment (Table 2). With these parameters, the prosthesis is then exposed by vaporisation of the soft tissue surrounding it (FIG. 6).

|
|
FIG 7. Platinum teflon piston swollen mushroom-like after direct CO2 laser irradiation with high power density (32,000 W/cm2, power 8 W, pulse duration 0.05 s). |
In the case of a wire/connective-tissue prosthesis (e.g. made of platinum), even direct lasering of the prosthesis is harmless. For a piston with teflon parts (e.g., platinum teflon piston), direct irradiation of the prosthesis must be avoided, since the teflon cannot withstand high temperatures (>300°C) of the laser irradiation, and its surface swells up mushroom-like without disintegration or inflammation (FIG. 7).
By non-contact vaporisation of the connective-tissue bands, the prosthesis is exposed without mechanically traumatising the inner ear. The soft tissue covering the oval niche is then symmetrically and extensively vaporised until the lateral borders of the oval window can be identified exactly. If the prosthesis is still situated within this connective tissue, the vaporisation is continued until it is completely freed from it. Only when all connective-tissue bands to its distal end have been separated is the prosthesis extracted from the site after disconnection from the incus with a 2 mm long 90° hook. If vertigo occurs (during interventions under local anaesthesia), the surgeon must interrupt the manipulations immediately and again check the distal end of the prosthesis for residual connective tissue bands.
In the centre of the oval window, a stapedotomy opening 0.5 to 0.7 mm in diameter is created by uniform vaporisation of the tissue until the perilymph of the vestibulum is identified. Depending on the findings (connective-tissue neomembrane and/or bony stapes footplate), powers of 1 W to 6 W (0.05 s) are required with a beam diameter of 0.18 mm and multiple juxtapositioned, slightly overlapping applications (6 to 12 applications). Using the one shot application technique of laser irradiation with rotating mirrors (SurgiTouch), powers of 4 to 22 W and pulse durations of 0.03 to 0.05 s are required.The prosthesis length is determined precisely (usually 4.5 to 4.75 mm) by measuring the distance between the vestibulum and the lower surface of the incus and adding 0.2 mm. To reduce the risk of renewed prosthesis migration, the prosthesis should project 0.1 to 0.2 mm into the stapedotomy opening. The platinum teflon piston is then inserted in the perforation and, if the incus is intact, fixed to the incus neck. In the case of a completely eroded incus, a malleo-vestibulopexy is performed to restore ossicular continuity.
Finally, the oval niche is sealed with connective tissue or a blood clot.
|
|
|
FIG 8a, 8b. Mean bone conduction threshold preoperatively and 3 to 6 months postoperatively: a) of patients treated with CO2 laser stapedotomy with primary surgery; b) of patients treated with revision CO2 laser stapedotomy |
Discussion
The advantages of stapedotomy compared to stapedectomy have already been confirmed by numerous authors (7,12,59,60,69,81,82,etc.). All studies demonstrate that stapedotomy causes fewer inner ear damages and less vertigo than conventional stapedectomy. Despite these advantages, it is nevertheless difficult to create a precise, round stapedotomy opening with mechanical instruments (drill, perforator). A partially fixed stapes is often accidentally mobilised by the manipulations (floating footplate) and a thin footplate not infrequently fractured. Perforation of a thick footplate obliterating the oval niche (obliterative otosclerosis) with the drill can cause significant inner ear trauma through vibrations.
In revision stapedectomy, conventional surgical procedures not infrequently lead to unsatisfactory hearing results and innerear damages. Studies by numerous ear surgeons have shown that a successful closure of the air-bone gap of less than 10 dB could be achieved only in less than half the patients (9,16,55,78). These studies indicate that 8 to 33% of the patients have poor hearing after revision operations. The incidence of a significant postoperative sensorineural hearing loss is 3 to 20% (up to 14% for profound sensorineural hearing losses).
Surgeons are warned particularly against damage to the inner ear through mechanical trauma due to excessive manipulations at the prosthesis and/or the connective tissue occluding the oval niche.
While exploring the middle ear for failed stapedotomy, the ear surgeon is in a dilemma. In order to find reasons for the existing conductive hearing loss, the operator must test the mobility and integrity of the entire chain of auditory ossicles and precisely assess the status of the oval window and the prosthesis position relative to the entrance of the vestibule. In this connection, he is frequently unable to determine the depth and lateral border of the oval window or to see the structures behind the connective tissue covering the oval niche.
While confining the palpation of these structures to a minimum in order to keep the inner ear trauma as mild as possible, the surgeon inevitably runs the risk of not recognising the exact cause of the existing conductive hearing loss (often more than one) and thus not initiating an adequate therapy of the hearing defect.
The old prosthesis should be removed very carefully; if vertigo occurs, it should be left in place in order to avoid permanent labyrinthine dysfunction or hearing loss. If extraction of the prosthesis is nevertheless achieved without appreciable traumatisation of the inner ear, the new prosthesis is inserted in the presumed centre of the oval niche.
If the oval window is free of residual disease and the surgeon has not caused any inner ear damage with his manipulations, the patients hearing will improve initially as a rule. The cause to which most failures after stapedotomy are ascribed, migration of the prosthesis, however, is frequently not eliminated by this. The new prosthesis can again migrate out of the oval niche. In view of these considerable difficulties in performing revision stapedectomies, the reported success rates of 30 to 50% are rather incomprehensible.
Laser stapedotomy, on the other hand, when performed with the suitable wavelength and the effective and safe parameters, enables the ear surgeon to create, by precise and non-contact vaporisation, a circular perforation in the stapes footplate regardless of its thickness or degree of fixation without mechanically traumatising the inner ear.Prior to the clinical application of the laser, extensive laboratory studies had to be performed in order to determine the ideal wavelength of laser radiation for stapedotomy and to establish the effective and safe laser parameters for each type of laser.
The results of previous studies support the usage of both visible (argon and KTP) and invisible, far infrared (CO2) laser systems for primary otosclerosis surgery (1-3,5,6,10,18,22,24,48,49,53,57,61,67,68,74,76,79,88).
Use of laser for revision surgery offers also distinct advantage over the conventional method. The complication rate is low and the statistically significant, improved success rate, independent of the laser system used (17,19,25,49,53,57,80,93,etc.). Measured as closure of air-bone gap of 20 dB or less, the rate of success with the laser ranges from 70% to 92% for laser surgery, compared to 49% to 85% for that of the conventional technique.
|
|
|
FIG 9a, 9b. Distribution of the patients with a postoperative air bone gap (average of 0.5 kHz, 1 kHz, 2 kHz and 3 kHz for air-conduction minus the average for bone conduction) of 0-10 dB, 11-20 dB, 21-30 dB or >30 dB with follow up of at least on year postoperatively: a) of patients treated with CO2 laser stapedotomy with primary surgery; b) of patients treated with revision CO2 laser stapedotomy. |
The authors have used the CO2 laser for stapedotomy. The results so far clearly document that the incidence and severity of postoperative complications after CO2 laser stapedotomy are lower than after conventional interventions (31,38,39,43.48).
In authors experience of almost 400 stapedotomies and more than 70 revision surgeries with the CO2 laser, there were no intra operative complications. In primary surgery postoperatively three patients (0.7%) showed significant sensorineural hearing loss, one patient (0.3%) a severe sensorineural hearing loss, which was probably caused by a granuloma and showed no improvement following the revision surgery. In revision surgery one patient (1.4%) developed a severe sensorineural hearing loss. Late cases of deafness were not observed. The mean sensorineural hearing losses before and after CO2 laser stapedotomy clearly show that there was no appreciable deterioration of inner ear function (FIG. 8a, 8b). A vestibular disturbance occurred in only eight cases because of the length of prosthesis. The postoperative air-bone gap closure in primary laser stapedotomy is comparable to that following conventional surgery (FIG. 9a). The hearing results obtained after revision stapedotomy so far suggest an improvement of the air-bone gap and an elimination of a significant hearing loss (FIG. 9b). These results are similar to the results of Lesinski and Newrock and Lesinski and in over 200 CO2 laser stapedotomies and stapedectomy revisions (52,53).
In revision stapedotomy, the CO2 laser provides the ear surgeon with three important advantages compared to the conventional technique: 1. improved diagnostic precision; 2. the possibility of better stabilisation of the new prosthesis in the centre of the oval niche; and 3. reduction of the inner ear trauma.
Thus, the CO2 laser enables the ear surgeon to eliminate a sound conduction hearing loss recurring after stapedotomy with high precision and safety. Some of the revision operations could only be performed by using the laser.
For the operative procedure, this means:1) CO2 laser stapedotomy is already performed at first interventions in order to minimise the risk of prosthesis migration, which is by far the most frequent cause for recurrence of a sound conduction hearing loss after stapedotomy or stapedectomy.
2) In order to avoid erosions of the incus, which are frequently the result of prosthesis migration and fixation with the bone surrounding the oval niche, a revision should be performed soon after a significant sound conduction hearing loss has been detected, and
3) A stapedotomy of the neomembrane of the oval window should always be performed. Three reasons argue in favour of this:
a) The covering neomembrane frequently conceals a residually fixed stapes footplate,b) The depth of the oval niche can be precisely ascertained and the length of the prosthesis exactly determined, and
c) The stapedotomy opening stabilises the new prosthesis in the centre of the oval window and minimises the risk of renewed migration.
Thus the CO2 laser appears to be well suited for application in stapes surgery. It does not endanger the inner ear with the laser parameters limited as specified. The one shot stapedotomy which is able to achieve an adequately large (0.5 to 0.7 mm in diameter) circular footplate perforation with a single application of laser irradiation without appreciable thermic damage to the surrounding area is a great advantage in CO2 laser stapedotomy.Application of the laser in stapes surgery contributes to the optimisation of this high-precision intervention and shows promise of improving hearing results and reducing the incidence of inner ear damages. Its performance in obliterative otosclerosis and in revision stapedotomy is superior to the conventional surgical technique.
REFERENCES
Antonelli PJ, Gianoli GJ, Lundy LB, et al. Early post-laser stapedotomy hearing thresholds. Am J Otol 1998;19(4):443-6.
Bartels LJ: KTP laser stapedotomy: is it safe? Otolaryngol Head Neck Surg 1990;103:685-92.
Beatty TW, Haberkamp TJ, Khafagy YW, Bresemann JA. Stapedectomy training with the carbon dioxide laser. Laryngoscope 1997;107:1441-4.
Bretlau P. Argon laser stapedotomy vs. Erbium laser stapedotomy. Otology 2000, XXII Annual Meeting of the Politzer Society, Zürich (1999)
Buchman CA, Fucci MJ, Roberson JB Jr, De La Cruz A: Comparison of argon and CO2 laser stapedotomy in primary otosclerosis surgery. Am J Otolaryngol 2000;21(4):227-30.
Causse JB, Gherini S, Horn KL: Surgical treatment of stapes fixation by fiberoptic argon laser stapedotomy with reconstruction of the annular ligament. Otolaryngol Clin North Am 1993;26(3):395-416.
Causse JR, Causse JB, Bel J. Amélioration de laudition en fonction du type de platinectomie ou de platinotomie effectué dans la chirurgie de lotospongiose. Ann Oto-Laryngol (Paris) 1985;102:401-5.
Charlton A, Dickinson MR, King TA, et al. YAG and holmium:YAG laser ablation of bone. Lasers Med Sci 1990;5:365-73.
Crabtree JA, Britton B, Powers WH. An evaluation of revision stapes surgery. Laryngoscope 1980;90:224-7.
DiBartolomeo JR, Ellis M. The argon laser in otology. Laryngoscope 1980;90:1786-96.
DiBartolomeo JR. Argon and CO2 lasers in otolaryngology: Which one, when, and why? Laryngoscope 1981;91(Suppl 26):1-16.
Fisch U. Stapedotomy versus stapedectomy. Am J Otol 1982;4(2):112-7.
Fischer R, Schönfeld U, Jovanovic S, Scholz C. Experimenteller Vergleich zwischen kurzgepulsten und kontinuierlich strahlenden Lasern in der Stapeschirurgie - akustische und thermische Ergebnisse. Arch Otorhinolaryngol 1990;(Suppl)2:224-7.
Fischer R, Schönfeld U, Jovanovic S, Jaeckel P. Thermische Belastung des Innenohres durch verschiedene Lasertypen bei der Laser-Stapedotomie. Arch Otorhinolaryngol 1992;(Suppl)2:251-3.
Gantz BJ, Jenkins HA, Kishimoto S, Fisch U. Argon laser stapedotomy. Ann Otol Rhinol Laryngol 1982;92:25-6.
Glasscock M: Revision stapedectomy surgery. Otolaryngol Head Neck Surg 1987;96:141-8.
Gherini SG, Horn KL, Bowman CA, Griffin GM. Small fenestra stapedotomy using a fiberoptic hand-held argon laser in obliterative otosclerosis. Laryngoscope 1990;100:1276-82.
Gherini S, Horn KL, Causse JB, McArthur GR. Fiberoptic argon laser stapedotomy: is it safe? Am J Otol 1993;14(3):283-9.
Haberkamp TJ, Harvey SA, Khafagy Y. Revision Stapedectomy with and without the CO2 Laser: An Analysis of Results. Am J Otol 1996;17:225-9.
Häusler R, Schar PJ, Pratisto H, et al. Advantages and dangers of erbium laser application in stapedotomy. Acta Otolaryngol 1999;119(2):207-13.
Häusler R: Fortschritte in der Stapeschirurgie. Laryngo-Rhino-Otol 2000;79(Suppl 2):95-139.
Hodgson RS, Wilson DF. Argon laser stapedotomy. Laryngoscope 1991;101:230-3.
Hommerich CP, Schmidt-Elmendorff A. Experimentelle CO2-, Holmium:YAG- und Erbium:YAG-Laseranwendung an der Steigbügelfußplatte. Eur Arch Otorhinolaryngol 1993;(Suppl 2):39-40.
Horn KL, Gherini S, Griffin GM. Argon laser stapedectomy using an Endo-Otoprobe system. Otolaryngol Head Neck Surg 1990;102:193-8.
Horn KL, Gherini S, Franz DC. Argon laser revision stapedectomy. Am J Otol 1994;15:383-8.
Jovanovic S, Scholz C, Berghaus A, Schönfeld U: Experimenteller Vergleich zwischen kurzgepulsten und kontinuierlich strahlenden Lasern in der Stapeschirurgie - histologisch-morphologische Ergebnisse. Arch Otorhinolaryngol 1990;(Suppl 2):72-3.
Jovanovic S, Berghaus A, Schönfeld U, Scherer H. Bedeutung experimentell gewonnener Daten für den Klinischen Einsatz verschiedener Laser in der Stapeschirurgie. Eur Arch Otorhinolaryngol 1991;(Suppl 2):278-80.
Jovanovic S, Prapavat V, Schönfeld U, et al. Experimentelle Untersuchung zur Optimierung der Parameter verschiedener Lasersysteme zur Stapedotomie. Lasermedizin 1992a;8:174-81.
Jovanovic S, Berghaus A, Scherer H, Schönfeld U. Klinische Erfahrungen mit dem CO2-Laser in der Stapeschirurgie. Eur Arch Otorhinolaryngol 1992b;(Suppl 2):249-50.
Jovanovic S, Anft D, Schönfeld U, et al. Tierexperimentelle Untersuchungen zur Eignung verschiedener Lasersysteme für die Stapedotomie. Eur Arch Otorhinolaryngol 1993a;(Suppl 2):38-9.
Jovanovic S, Schönfeld U, Fischer R, Scherer H: CO2 laser in stapes surgery. Proc SPIE 1993b;1876:17-27.
Jovanovic S, Schönfeld U, Fischer R, Döring M, Prapavat V, Müller G, Scherer H: Temperaturmessungen im Innenohr-Modell bei Laserbestrahlung. Lasermedizin 1995a;11:11-8.
Jovanovic S, Anft D, Schönfeld U, et al. Tierexperimentelle Untersuchungen zur CO2-Laser-Stapedotomie. Laryngo-Rhino-Otol 1995b;74:26-32.
Jovanovic S, Schönfeld U, Prapavat V, et al. Die Bearbeitung der Steigbügelfußplatte mit verschiedenen Lasersystemen. Teil I: Kontinuierlich strahlende Laser. HNO 1995c;43:149-58.
Jovanovic S, Schönfeld U, Prapavat V, et al. Die Bearbeitung der Steigbügelfußplatte mit verschiedenen Lasersystemen. Teil II: Gepulste Laser. HNO 1995d;43:223-33.
Jovanovic S, Schönfeld U, Fischer Ret al. Thermische Belastung des Innenohres bei der Laser-Stapedotomie. Teil I: Kontinuierlich strahlende Laser. HNO 1995e;43:702-9.
Jovanovic S, Anft D, Schönfeld U, et al. H: Experimental studies on the suitability of the erbium laser for stapedotomy in an animal model. Eur Arch Otorhinolaryngol 1995f;252:422-8.
Jovanovic S, Schönfeld U. Application of the CO2 laser in stapedotomy. Adv Oto-Rhino-Laryngol 1995g;49:95-100.
Jovanovic S. Der Einsatz neuer Lasersysteme in der Stapeschirurgie. In: Müller GJ, Berlien HP (eds). Fortschritte der Lasermedizin., Landsberg: Ecomed, 1996a, 14.
Jovanovic S, Schönfeld U, Fischer R, et al. Thermische Belastung des Innenohres bei der Laser-Stapedotomie. Teil II: Gepulste Laser. HNO 1996b;44:6-13.
Jovanovic S, Schönfeld U, Prapavat V, et al. Effects of continuous wave laser systems on stapes footplate. Las Surg Med 1996c;19:424-32.
Jovanovic S, Schönfeld U, Scherer H. CO2 Laser in Revision Stapes Surgery. SPIE Proceed 1997a;2970:102-8.
Jovanovic S, Schönfeld U, Hensel H, Scherer H. Clinical experiences with the CO2 laser in revision stapes surgery. Lasermedizin 1997b;13:37-40.
Jovanovic S, Schönfeld U, Prapavat V, et al. Effects of pulsed laser systems on stapes footplate. Lasers Surg Med 1997c;21:341-50.
Jovanovic S, Schönfeld U, Fischer R. Thermic effects in the vestibule during laser stapedotomy with pulsed laser systems. Lasers Surg Med 1998;23:7-17.
Jovanovic S, Anft D, Schönfeld U, et al. Influence of CO2 Laser Application of the Guinea-Pig Cochlea on Compound Action Potentials. Am J Otol 1999;20:166-73.
Jovanovic S, Jamali J, Anft D, et al. Influence of pulsed lasers on the morphology and function of the guinea-pig cochlea. Hearing Res 2000;144:97-108.
Jovanovic S. CO2 laser in Stapes Surgery. In: Jovanovic S, Levine H, Oswal V, Remacle M, eds. Principles and Practice of Lasers in Otolaryngology, Head and Neck Surgery Den Haag: Kugler Verlag, 2002:335-57.
Lesinski SG. Lasers for otosclerosis. Laryngoscope 1989;99(Suppl 46):1-24.
Lesinski
Lesinski
Lesinski SG, Stein JA. Lasers in revision stapes surgery. Oper Tech Otolyngol Head Neck Surg 1992;3:21-31.
Lesinski SG, Newrock R. Carbon dioxide lasers for otosclerosis. Otolaryngol Clin North Am 1993;26:417-41.
Lim RJ. Safety of carbon dioxide laser for stapes surgery. Lasers Surg Med 1992;(4):6.
Lippy WH: Stapedectomy revision. Am J Otol 1980;2:67-77.
Lyons GD, Webster DB, Mouney DF, Lousteau RJ. Anatomical consequences of CO2 laser surgery of the guinea pig ear. Laryngoscope 1978;88:1749-54.
McGee TM. The argon laser in surgery for chronic ear disease and otosclerosis. Laryngoscope 1983;93:1177-82.
McGee TM, Kartush JM. Laser stapes surgery (letter). Laryngoscope 1990;100:106-7.
Marquet J. Otosclerosis: Small hole technique. J Laryngol Otol 1983;(Suppl 8):78-80.
Marquet J. Stapedotomy technique and results. Am J Otol 1985;6:65-7.
Molony TB. CO2 laser stapedotomy. J La State Med Soc 1993;145(9):405-8.
Nagel D. Laser in der Ohrchirurgie. HNO 1996;44:553-4.
Nagel D. The Er:YAG laser in ear surgery: first clinical results. Lasers Surg Med 1997;21(1):79-87.
Nissen RL. Argon laser in difficult stapedotomy cases. Laryngoscope 1989;108:1669-73.
Nuss RC, Fabian RL, Sarkar R, Puliafito C. Infrared laser bone ablation. Lasers Surg Med 1988;8:381-91.
Palva T, Karja J, Palva A. Otosclerosis surgery. Acta Otolaryngol 1977;83:328-35.
Palva T. Argon laser in otosclerosis surgery. Acta Otolaryngol (Stockh) 1987;104:153-7.
Perkins RC: Laser stapedotomy for otosclerosis. Laryngoscope 1980;90:228-41.
Persson P, Harder H, Magnuson B. Hearing results in otosclerosis surgery after partial stapedectomy, total stapedectomy and stapedotomy. Acta Otolaryngol (Stock) 1997;117:94-9.
Pfalz R, Lindenberger M, Hibst R. Mechanische und thermische Nebenwirkungen des Argon-Lasers in der Mittelohrchirurgie (in vitro). Eur Arch Otorhinolaryngol 1991;(Suppl 2):281-2.
Pfalz R, Bald N, Hibst R. Eignung des Erbium:YAG Lasers für die Mittelohrchirugie. Eur Arch Otorhinolaryngol 1992;(Suppl 2):250-25.
Pfalz R. Eignung verschiedener Laser für Eingriffe vom Trommelfell bis zur Fußplatte (Er:YAG-, Argon-, CO2-s.p.-, Ho:YAG-Laser). Laryngo-Rhino-Otol 1995;74:21-5.
Pratisto H, Frenz M, Ith M, et al. Temperature and pressure effects during erbium laser stapedotomy. Lasers Surg Med 1996;18:100-8.
Rauch SD, Bartley ML. Argon laser stapedectomy: comparison to traditional fenestration techniques. Am J Otol 1992;13(6):556-60.
Schönfeld U, Fischer R, Jovanovic S, Scherer H. Lärmbelastung während der Laser-Stapedotomie. Eur Arch Otolaryngol 1994: (Suppl 2):244-6.
Shabana YK, Allam H, Pedersen CB. Laser stapedotomy. J Laryngol Otol 1999;113(5):413-6.
Shah KU, Poe DS, Rebeiz EE, et al. Erbium laser in middle ear surgery: in vitro and in vivo animal study. Laryngoscope 1996;106:418-22.
Sheehy JL, Nelson RA, House HP. Revision stapedectomy: A review of 258 cases. Laryngoscope 1981;91:43-51.
Silverstein H, Rosenberg S, Jones R. Small fenestra stapedotomies with and without KTP laser: a comparison. Laryngoscope 1989;99:485-8.
Silverstein H, Bendet E, Rosenberg S, Nichols M. Revision stapes surgery with and without laser: a comparison. Laryngoscope 1994;104:1431-8.
Smyth GDL, Hassard TH. Eighteen years experience in stapedectomy. The case for the small fenestra operation. Ann Otol Rhinol Laryngol (Suppl) 1978;87:3-36.
Somers T, Govaerts P, Marquet T, Offeciers E. Statistical analysis of otosclerosis surgery performed by Jean Marquet. Ann Otol Laryngol 1994;103:945-51.
Strunk CL, Quinn FB, Bailey BJ. Stapedectomy techniques in residency training. Laryngoscope 1992;102:121-4.
Thoma J, Unger V, Kastenbauer E. Temperatur- und Druckmessungen im Innenohr bei der Anwendung des Argon-Lasers. Laryngo-Rhino-Otol 1981;60:587-90.
Thoma J, Unger V, Kastenbauer E. Funktionelle Auswirkungen des Argon-Lasers am Hörorgan des Meerschweinchens. Laryngo-Rhino-Otol 1982;61:473-6.
Thoma J, Mrowinski D, Kastenbauer E. Experimental investigations on the suitability of the carbon dioxide laser for stapedotomy. Ann Otol Rhinol Laryngol 1986;95:126-31.
Vernick DM. Laser stapes surgery (letter). Laryngoscope 1990;100:106-7.
Vernick DM. A comparison of the results of KTP and CO2 laser stapedotomy. Am J Otol 1996;17:221-4.
Vollrath M, Schreiner C. Influence of argon laser stapedotomy on cochlear potentials. I. Alteration of cochlear microphonics (CM). Acta Otolarygol (Stockh) 1982a;(Suppl)385:1-31.
Vollrath M, Schreiner C. The effects of the argon laser on temperature within the cochlea. Acta Otolarygol (Stockh) 1982b;93:341-8.
Vollrath M, Schreiner C. Influence of argon laser stapedotomy on cochlear potentials. III. Extracochlear record DC potential. Acta Otolarygol (Stockh) 1983a;96:49-55.
Vollrath M, Schreiner C. Influence of argon laser stapedotomy on inner ear function and temperature. Otolaryngol Head Neck Surg 1983b;91:521-6.
Wiet RJ, Kubek DC, Lemberg P, Byskosh AT. A meta-analysis review of revision stapes surgery with argon laser: effectiveness and safety. Am J Otol 1997;18(2):166-71.
|
Pro Otology |
Journal Home Contents Preview Next |