|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 4, No 2-3:118121 © 2004
All rights reserved. Published by Pro Otology Association
Acute Mastoiditis with Exteriorization
the Forgotten Complication
R. Benchev, V. Pavlov, Zl. Zelyazkova
Medical Institute of the Ministry of Interior, ENT clinic
First United City Hospital Sofia, ENT clinic
ABSTRACT
Objective: The purpose of this study was to observe the pathophysiology, the clinical course, the management and the outcome of the mastoiditis as a complication of acute suppurative otitis media.
Study design: The study was a retrospective review of two cases with mastoiditis.
Setting: The study was performed in the Clinics of Otorhinolaryngology in Medical Institute Ministry of Interior and the First Multistructional State Hospital, Sofia.
Patients: The study included two patients with acute mastoiditis as a complication of acute suppurative otitis media, with exteriorization-neck phlegmona and neuritis of cranial nerves.
Interventions: Urgent surgical treatment - mastoidectomy with apex amputation, incision and drainage of the neck phlegmona and antibiotic treatment were performed.
Main outcome measures: The patients passed precise otorhinolaryngological examination, laboratory tests, bacteriological investigation, pure tone audiometry, X-ray examination, CT scan,
Results: After the infection was eradicated, the wounds were sutured. The general condition of the patients improved and they were discharged.
Conclusions: Although rarely met, mastoiditis is a complication, which should not be forgotten and should be considered in cases of severe, difficult to cure otitis, both in children and adults.
Key Words: Acute Mastoiditis, Phlegmona, Complication.
Pro Otology 2-3:118121, 2004
Introduction
Mastoiditis is a very rare complication of suppurative otitis media in the antibiotic era especially in adults. According to T. Palva, H. Virtanen, M. Kinen (1985), it is found in 0,004% of the cases with acute otitis media. In a survey of the literature in English from 1980 on, by Medline, we could not find a single case of an adult with mastoiditis reported. That is why; we describe two cases with mastoiditis in adults, complicated with neck phlegmona and neuritis of cranial nerves, as an extremely rare phenomenon nowadays.
Materials and Methods
Case 1.
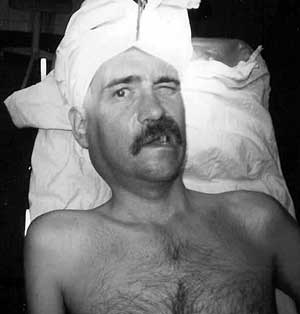
A 37 years old patient was admitted in the clinic in a state of emergency with severe, pulsating headache, profuse purulent discharge from the ear, high temperature up to 39 degree C, painful swelling of the right neck, immobility of the right half of the face, difficult movement of the head. The onset of the disease started about 4 weeks ago, but the swelling in the parotid area and the neck appeared 10 days ago and gradually increased. The patient has not looked for medical help and he treated himself with analgetics and vitamins. He systematically abused with alcohol.
|
|
At admission, the patient was in impaired general condition, with high temperature, but with clear mind. The blood pressure was 120/80 mm Hg, pulse frequency of 85/min. almost permanent purulent discharge from the right ear was found on the initial inspection. The lateral and posterior neck was swollen and painful and with hyperemic skin. The swelling reached about 5 cm from the clavicle, and when pressed, purulent discharge from the ear appeared (Lucs symptom). The right shoulder stayed lower than the left and the abduction of the right arm was more difficult. The head was compulsory bent to the right. The right facial half was with impaired mobility (paresis of peripheral type) (FIG. 1). The X ray examination of the mastoid did not reveal the characteristic signs of mastoiditis. The audiometry showed pure conductive hearing loss. The laboratory tests revealed leucocytosis of 15,2 g/l and ESR 110/130 mm. The bacteriological investigation showed St. aureus and anaerobes
|
|
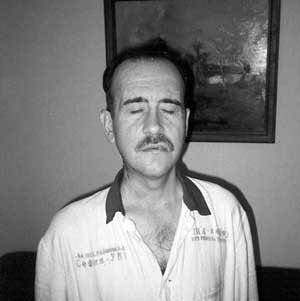
FIG. 3. Case 1. The patient after surgical treatment. |
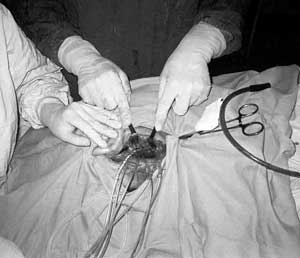
Urgent surgical treatment was carried out. Under general anesthesia mastoidectomy with apex amputation, incision and drainage of the neck phlegmona was done. Mastoid cavity was found full of easily bleeding granulations, and purulent secretion. No dehiscence or erosion of the osseous canal of the facial nerve was found. The purulent discharge passed through the mastoid tip under the stermomastoid muscle. Exteriorization in the zones of Bezold and Mouret was found. The abscess collection spread medially and posteriorly towards the cranial base and the vertebra, inferiorly along the carotid sheath, in front and behind the cervical spine. After the incision in front of the sternomastoid muscle, about 250ml pus was evacuated. Suction drains for constant suction and lavage were inserted (FIG. 2). The wound was left open for better aeration and clearance.
Antibiotic treatment with Penicillin, Amikacin and Metronidazol was started initially. On the next day the CT of the skull, petro-mastoid area and the neck showed that the infection persisted paravertebrally and towards the cranial base. The neck incisions were revised and additional drains in the affected areas were inserted.
The general condition of the patient gradually improved. After 10 days the antibiotic treatment continued with Lincomycin for another 7 days and was finished with Septrin. The drains were removed gradually. After the infection was eradicated the wound was sutured. The paresis of the VII and the XI cranial nerves subsided and the hearing became normal. The patient was discharged from the clinic in good health.
Case 2.
A 54 years old female with strong headache and painful swelling of the left side of the neck, high temperature up to 38,5 degree C and purulent discharge from the left ear was referred to the clinic. The initial symptoms were of earache since 3 weeks and purulent discharge from the left ear. The patient was seen by an otolaryngologist who began oral antibiotic treatment with Apicillin for 5 days. At first, the discharge decreased and stopped, but later, after the antibiotic was ceased, it began again. Two weeks later, a pulsating pain in the neck appeared, the temperature raised higher than 38 degree C, the general condition became impaired. The swelling on the left side of the neck increased and the movements of the head were very difficult. The purulent discharge from the ear became profuse. In such condition she was admitted in the clinic.
|
|
The examination revealed deep neck abscess reaching the supraclavicular region (FIG. 3). There was a swelling behind the left ear. The tympanic membrane had a large perforation with pulsating discharge. The X ray examination of the temporal bone and the neck showed purulent inflammation in the mastoid and lateropharyngeal abscess formation in the left side of the neck. The inflammation was not penetrating the mediastinum.
Surgical treatment was performed. Mastoidectomy with apex amputation and incision of the lateral neck was carried out (FIG. 4). The whole mastoid was full of purulent secretion and bone particles. Exteriorization in Bezolds area was found from where the pus slid under the sternomastoid muscle and spread along the cervical planes inferiorly up to the clavicle. After the incision, about 200 ml of pus was aspirated. Suction drains were inserted in the cervical wound (FIG. 5). The bacteriological findings showed mixed infection of St. aureus and anaerobes. Along with the surgical treatment, antibiotic treatment with Ceftriaxon and Metronidazol was started.
Gradually, the general and local condition improved and the drains were removed. The medical treatment continued with Clindamycin for another 10 days. The wound was sutured and the patient was discharged from the clinic.
Discussion
The purulent mastoiditis is a complication of the acute suppurative otitis media and is manifested by bone destruction of the cells of the mastoid process, granulation tissue formation and purulent lakes. At the beginning the bone septa of the mastoid cells are destroyed, but later, with the formation of granulation tissue, destruction of the solid bone with fistulization and exteriorization of the purulent process is found. Mastoiditis is most common in childhood and sometimes is the first manifestation of the ear infection (1). In the antibiotic era it is a very rare complication, which is diagnosed rapidly and is frequently treated only medically (1,2,3). The exteriorization is an extreme exception. It usually appears in cases with very virulent infection, in low host defense and in untreated cases. Our first patient has not received adequate treatment for about 3 weeks, because he has not looked for medical help. The systematical alcohol abuse apparently has lowered his defensive forces. Sometimes, except exteriorization, central nerve system affection and development of sigmoid sinus thrombosis, sepsis and labyrinthitis could be found (5,7).
In both cases exteriorization through the zone of Bezold was found. In our first case the paresis of the VII and the XI cranial nerves was due to the exteriorization of the inflammatory process. In the break through Bezolds zone the pus passes medially from the sternomastoid muscle and spreads inferiorly under it. In Mourets exteriorization, the infection breaks the mastoid process in the area of the deep subantral and intersinusfacial cells and spreads medially from the digastric muscle towards the cranial base and the pharynx. The lesion of the facial nerve was extratemporal near the stylomastoid foramen, and the accessory nerve was affected by the infection after it leaves the jugular foramen. Here, commonly occur associated pareses of the IX, X, XI cranial nerves, but in our case no lesion of n. glossopharyngeus and n. vagus was found.
The palsy of the facial muscles and the trapezius and sternomastoid muscles passed after the surgical treatment. The mobility of the shoulder restored several days after the incision and the drainage of the neck, while the facial paresis recovered more slowly for about 40 days.
Some authors (1,2,3), in absence of subperiosteal abscess and central nerve system affection, recommend delay of the surgical treatment. They begin with intensive antibiotic treatment and wide myringotomy, and if there is no response to the management after 48 hours, surgery is performed. Other (4,7,8), prefer early mastoidectomy for the risk of intracranial complications. We consider that the early surgical treatment is to be preferred and in cases with exteriorization, it is without alternative. We think that the favorable outcome in our case is due exclusively to the aggressive surgical and massive antibiotic treatment. The wide mastoidectomy with amputation of the tip and connection of the post auricular and the neck incisions, play great part for the adequate drainage of the surgical wound. The suction system of drains for constant lavage and clearance of necrotic matters and the revisions of the cervical wound and mastoid cavity twice daily were of great importance as well.
Conclusions
Although rarely met, mastoiditis is a complication, which should not be forgotten and should be considered in cases of severe, difficult to cure otitis, both in children and adults. The adequate management in adults is wide mastoidectomy with exenterating of the whole cell system and amputation of the tip of the mastoid, but not only antrotomy, which is usually sufficient in children. The neck abscesses and phlegmonas due to the exteriorization are treated surgically according to the rules of the septic surgery. CT has great importance for the correct diagnosis and viewing of the spread of the infection.
REFERENCES
Harley E, Sdralis T, Berkovich R. Acute mastoiditis in children: a 12-year retrospective study. Otolaryngol Head Neck Surg 1997;116:26-30.
Herrmann P, Baumann A, Fanconi A. Acute mastoiditis: clinical, microbiological and therapeutic aspects. Eur J Pediatr 1990;149:560-4.
Ogle J, Laner B. Acute mastoiditis. Diagnosis and complications. Am J Dis Child 1986;140:1178-82.
Lautermann J, Liebermann B, Schaper J, Knauer-Fischer S. Mastoiditis in childhood. Klin Paediatr 1990;210:345-8.
Palminha J, Penha R. Acute mastoiditis in children. Acta Med Port 1998;11:643-7.
Palva T., Virtanen H, Klein JM. Acute and latent mastoiditis in children. J Laryngol Otol 1985;99:127-36.
Venezio F, Naidich T, Schulmann S. Complications of mastoiditis with special emphasis on venous sinus thrombosis. J Pediatr 1982;101:509-13.
Spodaryk et al. Mastoiritis a forgotten disease? Przegl Lek 1992;49:403-5.
|
Pro Otology |
Journal Home Contents Preview Next |