|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 4, No 2-3:7982 © 2004
All rights reserved. Published by Pro Otology Association
Is Tos Technique Safe? Distances from Dissection Margins of Tos Modified Canal Wall-up Mastoidectomy to Facial Nerve
Cem Uzun
Otorhinolaryngology Department, Trakya University Faculty of Medicine, Edirne, Turkey
ABSTRACT
Objective: Tos modified canal wall-up mastoidectomy (Tos technique) consists of otosclerosis drilling of the superoposterior bony annulus, transcanal atticotomy with preservation of thin bridge and cortical mastoidectomy with intact canal wall. The aim of the present study is to measure the distances from dissection margins of the Tos technique to facial nerve and to evaluate the dangerous steps of the technique.
Study Design: Six temporal bones of formalin fixed human cadavers, in which Tos technique was performed, were used for the study. Posterior canal walls were drilled down under an operating microscope, but very thin bony bridges were preserved just behind the original dissection (drilling of superoposterior bony annulus and atticotomy) margins. In addition, decompression of the tympanic and mastoid segment of the facial nerve was performed.
Setting: Otorhinolaryngology Department, Trakya University Faculty of Medicine, Edirne, Turkey
Main Outcome Measures: Shortest distances to facial nerve at four critical points (chordal eminence, corner over the second genu of the facial nerve, posteroinferior corner of the atticotomy and inferior edge of the atticotomy at the level of malleus neck) were measured.
Results: Overall, range of the shortest distance to facial nerve was 2 to 5mm. The shortest distance was at chordal eminence (mean: 2.92mm, median: 2.5mm, range: 2-4mm). The dissection margin at the site of drilling of superoposterior bony annulus was closer to the facial nerve than the inferior dissection margin of the atticotomy. At the level of bony annulus, the distance between the facial nerve and the inferior margin of atticotomy became shorter from anterior to posterior. The mean distance to facial nerve at the inferior edge of atticotomy at the level of malleus neck was 4.58mm versus 4.17mm at the posteroinferior corner of atticotomy.
Conclusions: Drilling of superoposterior bony annulus might be the most dangerous step of the Tos technique because a surgeon could get very close to the facial nerve during drilling at this part. Compared to the classic canal wall-up and canal wall-down mastoidectomies, where drilling of the bone to the level of facial nerve is necessary, the Tos technique seems to be a safer technique. However, besides a thorough knowledge of surgical anatomy and recognizing the nerve during surgery, surgeons must be very careful to avoid facial nerve injury, especially during drilling transcanally at the posterior external ear canal and posteroinferior atticotomy region.
Key Words: Tos technique, Mastoidectomy, Temporal bone anatomy, Facial nerve, Complication.
Pro Otology 2-3:7982, 2004
INTRODUCTION
Tos canal wall-up mastoidectomy (Tos technique) is also known as modified combined-approach tympanoplasty or modified intact canal wall technique (1-7). Tos modified combined-approach tympanoplasty in 1970, mainly to avoid second look operations and revisions, which usually end in a canal wall-down procedure (1,5). The principle of this modified technique is to create such conditions in the attic that the retraction does not necessarily lead to recurrent cholesteatoma requiring re-operation, but most often to a peaceful, small cavity with an acceptably wide access (2).
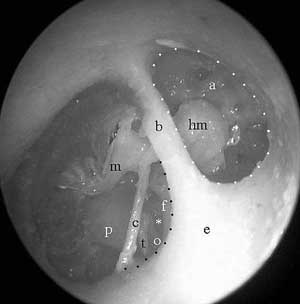
Tos technique consists of otosclerosis drilling of the superoposterior bony annulus (transcanal posterior tympanotomy), transcanal atticotomy opening with preservation of thin bridge and cortical mastoidectomy with preservation of a thin posterior bony ear canal wall (FIG. 1) (1-7). Drilling of superoposterior bony annulus ensures good visualization of tympanic sinus, and atticotomy gives fine view of anterior attic, which are the two most frequent location of residual cholesteatoma (2,5,8,9).One of the most feared complications in otologic surgery is iatrogenic injury to facial nerve. Thus, safety of a surgical technique for complete cholesteatoma removal mainly depends on the safety of the approach to the disease and how safe the dissection is without disturbing the facial nerve.
The aim of the present study is to measure the distances from dissection margins of the Tos technique to the facial nerve and to evaluate the dangerous steps of the technique. It is hoped that the information here will assist the otologic surgeon, who performs Tos technique as well as other techniques in which transcanal posterior tympanotomy and/or atticotomy are done.
MATERIAL AND METHODS
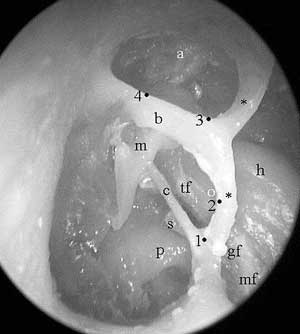
Six temporal bones of formalin fixed human cadavers, in which Tos modified canal wall-up mastoidectomy was performed were used for the study. These temporal bones had been used for another study, in which visualization of structures in the middle ear via Tos modified canal wall-up mastoidectomy was compared to the visualization via classic canal wall-up and canal wall-down mastoidectomies (10). For the present study, intact canal walls of these temporal bones with Tos technique were drilled down under an operating microscope, but very thin (about 1 mm wide) bony bridges were preserved just behind the original dissection (drilling of superoposterior bony annulus and atticotomy) margins (FIG. 2). Decompression of the tympanic and mastoid segment of the facial nerve was also performed in all temporal bones (FIG. 2). Shortest distances to facial nerve at four critical points (chordal eminence, corner over the second genu of the facial nerve, posteroinferior corner of the atticotomy and inferior edge of the atticotomy at the level of malleus neck; FIG. 2, FIG. 3), where a surgeon could get closer to facial nerve during drilling/dissection, were measured (FIG. 3) by using custom made millimetric tapes under high magnification of an operating microscope. When represented in clock positions, these critical points were at 9, 10, 11 and 12 oclock positions in the right ear and at 3, 2, 1 and 12 oclock positions in the left ear, respectively.
RESULTs
Shortest distances to facial nerve at four dissection-margin points (FIG. 2, FIG. 3) are shown in the Table. The measured distances range between 2 and 5 mm. The shortest distance was at chordal eminence, where, according to the measurements, a surgeon could get closer to facial nerve as near as 2 mm (mean: 2.92 mm, median: 2.5 mm, range: 2-4 mm). The dissection margin at the site of drilling of superoposterior bony annulus (otosclerosis drilling) was closer to the facial nerve than the inferior dissection margin of the atticotomy (Table 1). At the level of bony annulus, the distance between the facial nerve and the inferior margin of atticotomy (just superior margin of the intact bridge) (FIG. 2, FIG. 3) became shorter from anterior to posterior. The mean distance to facial nerve at the inferior edge of atticotomy at the level of malleus neck was 4.58 mm, which was longer than the one at posteroinferior corner of atticotomy (4.17 mm) (Table 1).
DISCUSSION
|
|
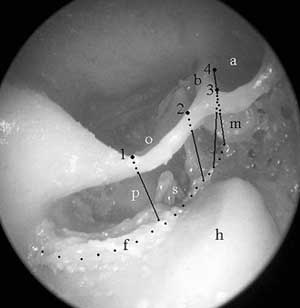
FIG. 3. The measured shortest distances (black lines) to facial nerve (f: black dots) from four critical points (1: chordal eminence; 2: corner over the second genu of the facial nerve; 3: posteroinferior corner of the atticotomy; and 4: inferior edge of the atticotomy at the level of malleus neck). View from posterior (mastoidectomy) to anterior at annular level. Incus has been removed. o: otosclerosis drilling, a: atticotomy, b: bony bridge, m: malleus, p: promontorium, s: stapes, h: horizontal semicircular canal. |
Iatrogenic injury to facial nerve in otologic surgery can be as high as 1% in primary procedures and higher in revision operations (11,12). The main reason for the injury has been reported to be the surgeons lack of familiarity with the surgical anatomy and unrecognizing the facial nerve (3).
When compared with the classic canal wall-up mastoidectomy, one of the most important advantages of Tos technique is that removal of cholesteatoma from the tympanic sinus is safer and easier after drilling of the posterior wall of the bony annulus (otosclerosis drilling) (2,3,5). In addition, most of the otology surgeons have extensive experience of operating on the stapes and footplate through this direct route. However, it was found in the present study that otosclerosis drilling step of the technique might be the most dangerous step because a surgeon could get closer to the facial nerve during drilling at this part nearer than he or she could do at the other parts of the dissection. The distance to facial nerve from the otosclerosis drilling could be as short as 2 or 3 mm, inferior part (at chordal eminence) being the shortest. Although the number of studied temporal bones (6 specimens) was small in the present study, this finding was in accordance with previous studies (14,15). In their morphometric analysis, Aslan et al have found that the mean distance between external auditory canal and facial nerve is 2.9 mm, which is similar with our value, 2.92 mm, at chordal eminence (15). However, Agirdir et al have found shorter distances (the shortest one was 0.83 mm) from annulus tympanicus to facial nerve, especially at bony posteroinferior wall of the external auditory canal (16). They have indicated that facial nerve position in relation to the annulus is variable and the nerve is most vulnerable to injury in the posteroinferior quadran (16). Facial nerve injury due to iatrogenic trauma has been most commonly observed after mastoidectomy procedures (13). This possibility of facial nerve injury may cause an otologic surgeon to work as far as possible from the nerve, thus causing an inadequate mastoid surgery (15). If he or she performs a canal wall-down mastoidectomy, he may leave more bone over the mastoid segment of the facial nerve resulting high facial ridge, which is one of the most important factors related to unsuccessful outcome of the open-technique procedures (15,17). Similarly, if a surgeon performs a canal wall-up mastoidectomy, because of the same reason (fear of facial nerve injury), he or she may not perform posterior atticotympanotomy, which, again, would result a poor outcome. This can be one of the important reasons why the frequency of residual cholesteatoma in Tos technique is considerably lower than that in classic combined-approach tympanoplasty (2,3,8,9,18-20). Transcanal atticotomy, one of the steps of the Tos technique, provides an opportunity for a direct survey of the anterior attic, this being the second most frequent location of residual cholesteatoma (2,5). When drilling over the lateral attic wall, special care must be taken at posteroinferior corner of the atticotomy, where is the nearest part of the atticotomy dissection to the facial nerve. We found that the mean distance to the facial nerve at posteroinferior corner of the atticotomy was 4.17 mm while the mean distance at the inferior edge of the atticotomy at the level of malleus neck was 4.58 mm (Table 1). When working deeply at the anterior attic near cog, care should also be taken not to make injury to the facial nerve.| Table 1. Shortest distances from dissection margins of the Tos technique to facial nerve. |
|
ACKNOWLEDGEMENTS
The author thanks Asim Aslan, MD, Associate Professor, Otorhinolaryngology Department, Celal Bayar University, Manisa, Turkey and Tunc Kutoglu, MD, Assistant Professor, Anatomy Department, Trakya University Faculty of Medicine, Edirne, Turkey, for their advices and help in the study.
REFERENCES
Tos M. Die operative therapie der chronischen otitis und des mittelohrcholesteatoms mit erhaltung der hinteren gehörgangswand (intact wall technique). HNO 1978;26:217-23.
Tos M. Modification of combined-approach tympanoplasty in attic cholesteatoma. Arch Otolaryngol 1982;108:772-8.
Tos M. Modification of intact canal wall technique in the treatment of cholesteatoma. Adv Otorhinolaryngol 1987;37:104-7.
Tos M, Lau T. Attic cholesteatoma. Recurrence rate related to observation time. Am J Otol 1988;9:456-64.
Tos M. Manual of middle ear surgery. Vol 2: Mastoid surgery and reconstructive procedures. Stuttgart: Thime, 1995:106-155,156-95.
Uzun C. Tos technique (modified combined-approach tympanoplasty) [Turkish]. Presented in the II. Trakya ENT Days New Advances in Otology Symposium, 8-9 September 2001, Edirne, Turkey.
Uzun C. Tos technique (modified combined-approach tympanoplasty) and reconstruction with palisade cartilage. Pro Otology 2002;2:22-5.
Glasscock ME, Miller GW. Intact canal wall tympanoplasty in the management of cholesteatoma. Laryngoscope 1976;86:1639-57.
Smyth GD. Postoperative cholesteatoma in combined approach tympanoplasty. Fifteen year report on tympanoplasty. Part I. J Laryngol Otol 1976;90:597-621.
Uzun C, Kutoglu T. Assessment of visualization of structures in the middle ear via Tos modified canal wall-up mastoidectomy versus classic canal wall-up and canal wall-down mastoidectomies. Submitted Int J Pediatr Otorhinolaryngol 2004.
Schuring AG. Iatrogenic facial nerve injury. Am J Otol 1988;9:432-3.
Wiet RJ. Iatrogenic facial paralysis. Otolaryngol Clin North Am 1982;15:773-80.
Green Ld, Shelton C, Brackmann DE. Iatrogenic facial nerve injury during otologic surgery. Laryngoscope 1994;104:922-6.
Adad B, Rasgon BM, Ackerson L. Relationship of the facial nerve to the tympanic annulus: a direct anatomic examination. Laryngoscope 1999;109:1189-92.
Aslan A, Goktan C, Okumus M, Tarhan S, Unlu H. Morphometric analysis of anatomical relationships of the facial nerve for mastoid surgery. J laryngol Otol 2001;115:447-9.
Agirdir BV, Sindel M, Yildirim FB, Derin A, Balkan EI. Anatomic relations between facial nerve and tympanic annulus. In: Magnan J, Chays A, eds. Proceedings of the sixth international conference on cholesteatoma and ear surgery. Marseille: Label Production, 2000:601-5.
Ozgirgin ON, Aydin E, Ozcelik T, Ozluoglu LN. Factors that affect the outcome of open-technique procedures performed in the treatment of cholesteatoma. Kulak Burun Bogaz Ihtis Derg 2003;10:47-50.
Lau T, Tos M. Treatment of sinus cholesteatoma. Long-term results and recurrence rate. Arch Otolaryngol Head Neck Surg 1988;114:1428-34.
Lau T, Tos M. Tensa retraction cholesteatoma: treatment and long-term results. J Laryngol Otol 1989;103:149-57.
Tos M, Lau T. Late results of surgery in different cholesteatoma types. ORL 1989;51:33-49.
|
Pro Otology |
Journal Home Contents Preview Next |