|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 2, No 1:34-36 © 2002
All rights reserved. Published by Pro Otology Association
Bilateral Congenital Ossicular Malformations, Combined with Fenestral Otosclerosis. Case Report
K. Kunev, N. Tsakov
Department of Otorhinolaryngology, University Hospital "Queen Joanna", Sofia, Bulgaria
ABSTRACT
Objective: Bilateral congenital ossicular malformations, combined with fenestrial otosclerosis - possibilities for earlier diagnosis and treatment.
Study design: The study design was a retrospective case review.
Setting: I ENT Clinic, MBAL "Tsaritsa Ioanna", Medical University - Sofia, Bulgaria.
Patient: A 15-year-old girl with bilateral conductive hearing loss, established soon after delivery.
Main outcome measure: These included clinical development, diagnosis and treatment of patient.
Results: Intraoperative findings revealed absence of incus, anomaly stapes with fenestrial otosclerotic fixation of basis at the oval niche in both ears. After operation the hearing of the patient was improved dramatically.
Conclussion: Though rare, congenital ossicular malformations are at great interest to the ENT clinicians.Early recognition of such disorders improves diagnosis and makes curable strategies more effective.
Key Words: COA - Congenital ossicular malformation, Fenestrial otosclerosis, Earlier diagnosis.
Pro Otology 1: 34-36, 2002
INTRODUCTION
Ossicular anomalies and resulting conducting deficit are commonly associated with external auditory canal dysplasia. Congenital ossicular anomalies (COA) without accompanying external ear malformations are less common (5).
There are also middle ear abnormalities among patients with bilateral otosclerosis, which could potentially affect successful stapedectomy, and the rates of success in these patients, including the chance of overclosure in the second ear.
Krieger LW, Lippy WH in "The other ear: findings and results in 1,800 bilateral stapedectomies" have concluded that abnormalities presented bilaterally were found in 135 patients - 7%. With otosclerosis requiring an oval window drillout as the most common finding 41% and followed by dehiscent or overhanging facial nerves (25%). In our case, there were full bilateral absences of incus (4).
Embryology
Maleus The cartilaginous precursor of the malleus originates as part of the dorsal end of Meckel`s cartilage. Excepting its anterior process, it ossifies from a single endochondral centre, which appears near the future neck of the bone in the fourth month in utero. The anterior process ossifies separately in dense connective tissue and joints the rest of the bone at about the six month of fetal life.
Incus The incus has a cartilaginous precursor continuos with the dorsal extremity of Meckel`s cartilage. Ossification often spreads from a single centre in the upper part of its long process in the fourth fetal month. The lenticular process, however, may have a separate centre.
Stapes The stapes is performed in the perforated end dorsal moiety of the hyoid arch cartilage of the fetus. Ossification starts from a single endochondral centre, appearing in the base in the fourth fetal month and then gradually spreads through the limbs of the stapes to fuse its body.
At the birth the auditory ossicles have reached an advanced state of maturity (6).
Clinical presentation and differential diagnosis
Conductive hearing loss is the predominant symptom, and fenestral otosclerosis is usually the major differential diagnostic consideration. The lack of progression of the hearing loss and the early age at diagnosis, such as seen in the case presented here, may indicate COA.
When the anomalies are bilateral, they are usually inherited via autosomal dominant transmission (1). There are several named syndromes associated with congenital conductive deficit secondary to ossicular derangement in those patients.
If the anomaly is unilateral, it is likely to be sporadic and isolated. Isolated COA are classified as follows:
· Incudostapedial disconnection;
· Malleus or incus fixations to the walls of the middle ear;
· Fixation of malleus, and incus and stapes fixation (2);
The least common category of COA is that which includes malleus and incus fixations. Although these anomalies are common when associated with external auditory canal dysplasias, they are uncommon as an isolated anomaly (1).
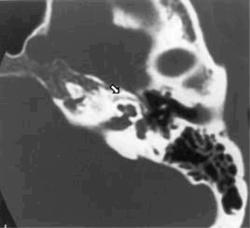
Computed tomography is the most accurate diagnostic tool for identifying COA preoperatively (Fig.1).
CLINICAL CASE
15-year-old girl with bilateral conductive hearing loss, which as we lately cleared was already, presented soon after delivery. Her mother didn't realize the problem until girl's 1-st birthday when she discovered the fact, that her doughtier did not react to voice signals coming from back. After consultation with ENT professional, the adenoids and tonsils were blamed for this condition and at 3.5 years (1990) those structures were operatively eradicated. An audiological assessment was tried to perform at that time, but with no success. At 1996 a second, audiological assessment was performed in Audiological Department of "Queen Joanna" University Hospital, Sofia.
The results have had showed that there was a bilateral conductive hearing loss with absence of stapedial reflex - findings bringing all the hallmarks of otosclerosis (Fig.1, Fig. 2).
The girl was suggested for hearing improve operation.
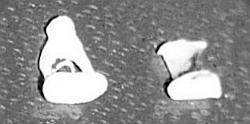
5 years later at 04 September her left ear was operated. At 04 April 2002 her right ear was operated too. These operations have had revealed equal pictures: absence of incus, anomaly stapes with fenestrial otosclerotic fixation of basis at the oval niche. The anomaly stapes has no caput and column, so tendon of stapedius muscle was attached to the fused crura (Fig. 3, Fig 4).
|
|
FIG. 2. The preoperative audiogram of the girl. |
CONCLUSSIONS
Though rare, congenital ossicular malformations are at great interest to the ENT clinicians. Early recognition of such disorders improves diagnosis and makes curable strategies more effective.
More over, the cumulated information from these clinical and intraoperative findings enriches our overall knowledge about the embryological disorders of middle ear development.
REFERENCES
Swartz JD, Harnsberger HR. Conductive hearing loss. In: Imaging of the Temporal Bone, 2nd Ed. New York: Thieme MedicalPublishers, 1992:131-4.
Valvassori GE, Mafee MF, Carter BL. Congenital anomalies of the temporal bone. In: Valvassori GE, Mafee MF, Carter BL, Imaging of the Head and Neck. New York: Thieme Medical Publishers, 1995:36-56.
Daniels RL. The speech chain. Am J of Otol 1999;78(4):8-11.
Krieger LW, Lippy WH. Hearing inpairrment of children. Am J of Otol 2000;21:30-3.
Michael K.J. Congenital hearing disability. ENT Journal 2001;128(9):15-7.
Gawton H.J. Nervous system, The ear, Auditory Ossicles. In: Gray`s Anatomy. Lippincot, 1996.
|
Pro Otology |
Journal Home Contents Preview Next |