|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 2, No 2:51-54 © 2002
All rights reserved. Published by Pro Otology Association
Cholesteatoma (Epidermoid Cyst) of the
Cerebellopontine Angle: Selecting the Surgical Approach
*J. Magnan, *A. Chays, †N. Girard, *M. Bruzzo, *R. Meller,
*S. Fuentes, *†M. Falcione, *†M. Sanna
*ORL, Hopital Nord, Marseille, France; †Radiology, Hopital Nord, Marseille, France
*†Gruppo Otologico, Via Emmanueli, Piacenza, Italy
ABSTRACT
Objective: The study presents the special features of managing cholesteatomas of the Cerebellopontine angle (CPA). Adaptation of surgical approaches to the tumor location and the extent of the lesions, the advantages of combining microsurgery with endoscopy control, the side effects of the interventions are discussed.
Study design: The experience with 11 cases of Cholesteatoma of the CPA.
Setting: ORL clinic.
Patients: 11 patients with cholesteatomas - 6 males and 5 females at the age from 11 to 76.
Interventions: MRI - preoperative and postoperative imaging assessement. Operative approaches according to tumor locations.
Main outcome measures: MRI and endoscopy control.
Results: The 11 operated patients with cholesteatoma of the CPA were treated successfully. The most common complications (6 with hearing loss, 5 with facial paralysis), connected to the location and the surgical approach to the tumors are discussed. Due to adherence with hidden and vital areas, fragments of the cyst wall left in 3 cases. 1 patient passed a second operation.
Conclusion: The complete removal, reducing the morbidity should be achieved through right surgical approach and endoscopy assisted microsurgery.
Key words: Cholesteatoma, Cerebellopontine angle, Surgical approach, Endoscopy assisted microsurgery.
Pro Otology 2: 51-54, 2002
Cholesteatomas or epidermoid cysts of the cerebellopontine angle are uncommon, congenital, non neoplastic, slowly growing lesions which arise from epithelial remnants during closure of the neural tube (1). So these lesions may occur anywhere along the neuraxis, but are most commonly located in the cerebellopontine angle (CPA) and parasellar region. As the cyst capsule often is adherent to the neurovascular structures, complete removal without additional deficit represents a challenging surgery. The surgical treatment is based on a carefully planned surgery including both right selection of the surgical approach, and combined microsurgical and endoscopic procedure.
MATERIAL AND METHODS
From 1992 to 1999 we treated 11 cholestatomas of the CPA, 6 males and 5 females with ages rarnging from 11 to 76, and with a mean age of 36.
Depending on the location of the cyst, a variety of symptoms may occur. The presenting symptoms are listed in Table 1.
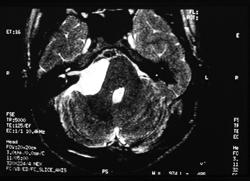
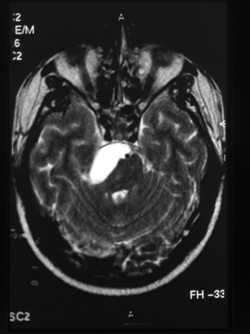
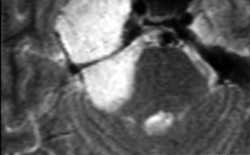
Magnetic resonance imaging (MRI) was and is the key assessment for diagnosis and for determining the full extension of the cyst. Epidermoid cysts typically appear isointense relative to cerebrospinal fluid (CSF) on T1, slightly hyperintense relative to CSF T2, with gadolinium. All our patients underwent preoperative and postoperative imaging assessment.
Tumor location (Table 2) was limited to the CPA in 4 cases (Fig. 1), anteriorly extended to the prepontine area in 2 cases (Fig. 2), medially extended to the IV ventricule in 1 case, with infra and supratentorial extension in 1 case, (Figs. 3,4), associated with petrous apex cholesteatoma in 3 cases (Fig. 5).
We noticed a harmonious distribution between right cerebellopontine cholesteatoma size (8 cases) and left petrous apex cholesteatoma size extending to the internal auditory canal and CPA (3 cases).
Surgical approaches
Controversies still persist over the appropriate surgical approach (Table 3). In selecting the surgical treatment it is of paramount importance to adapt our approach to the location and the extent of the lesion, and not to adapt the tumor removal to only one surgical approach.
In the 4 cases of cerebellopontine cholesteatoma, a retrosigmoid approach was used in 2 cases, transotic approach in 1 case, and a combined retrolabyrinthine subtemporal approach in 1 case. The side effects were: one partial removal, one hearing loss, 2 cases of facial weakness grade III and IV.
In the 2 cases of prepontine cerebellopontine cholesteatoma, a retrosigmoid approach was chosen in 1 case, and modified transcochlear approach in the other case. Complete removal was achieved, with one normal facial function and one case of grade III facial nerve weakness.
In the case of intraventricular cholesteatoma a transcochlear approach was performed. In the case of a huge cerebellopontine cholesteatoma with infra and supratentorial location we made a combined transcochlear - subtemporal - trans orbitozygomatic approach. A very tiny fragment of capsule was left behind and medial to the basilar artery. The complete facial rerouting recovered to a grade III facial function. A severe diplopia was the major side effect. In the 3 cases of apex cholesteatoma extended within the internal auditory canal (IAC) and/or CPA, an enlarged subtemporal approach was selected. One incomplete removal was performed due to the matrix of the cyst intimately adherent with the wall of the cavernous sinus. No postoperative facial paralysis occurred but there was pain and facial numbness in one case.
Out of 11 patients the overall complications (Table 4) were total hearing loss in 6 cases, facial paralysis in 4 cases, diplopia and pain in 1 case each. There was no aseptic meningitis.
Once the right selection of the surgical approach resolved, the second step is to obtain a total resection of the cholestatoma which is usually difficult without incurring injury to the involved neuro-vascular structures. Factors opposing total removal, are distant remnants and firm adhesions of tumor capsule (2), which represents a high risk of recurrence. In order to improve the management of the cholesteatoma removal we combined microsurgery and endoscopy. Endoscope value in otoneurology is well known and the main advantages of a complementary (3) endoscopic view are the following:
- panoramic and unobstructed view without being invasive
- look around the corner at the site of the disorder
- more comprehensive map of the neurovascular components.
Its application to cholesteatoma removal within the CPA is more than useful.
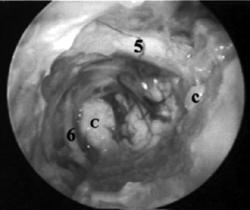
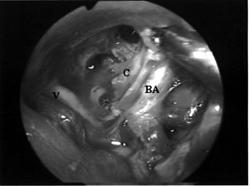
After meticulous microsurgical peeling of the matrix surrounding the keratine and adhering to the neural and vascular structures, the completeness of the surgical excision is confirmed endoscopically (Figs. 6,7).
Out of 11 patients operated on using endoscopy-assisted microsurgery, fragments of the cyst wall were left in 3 cases due to adherence with hidden and vital areas such as cavernous sinus, between the basilar artery and the brain stem. In the follow-up period, which ranged from 8 months to 5 years, one patient with incomplete removal experienced an obvious growth of residual fragments on the post-operative imaging assessment after two years. This patient was treated by a second operation without any additional side effect.DISCUSSION
Yasargyl et al. (4) and De la Cruz and Doyle (5) using suboccipital and transcochlear approaches respectively claimed complete removal of epidermoid cyst of the CPA in all cases. Other authors (6-8) published 25 % to 43 % of cases in which strong adhesion to the basilar artery and its branches and the cranial nerves prevented total tumor resection. Intentionally left fragments are responsible for recurrence in up to approximately 20 %. The mean time of recurrence was 32 months after surgery (9).
CONCLUSION
Right surgical approach and endoscopy as an adjuvant to microneuro-otologic surgery should increase the frequency of complete removal, reducing the morbidity.
|
|
REFERENCES
Cobbs C, Pitts L , Wilson C. Epidermoid and dermoid cyst of posterior fossa. Clin Neurosurg 1997;44:511-28.
Talacchi A, Sala F, Turazzi S, Bricolo A. Controversies in the management of posterior fossa epidermoids. In: M. Sanna. Acoustic Neurinoma and other CPA tumors. Monduzzi Editore, 1999:779-82.
Magnan J, Sanna M. Endoscopy in neuro-otology. Thieme 1999.
Yasargil G, Abernathey C, Sarioglu A. Microneurosurgical treatment of intracranial dermoid and epidermoid tumors. Neurosurgery 1989;24:561-7.
De La Cruz A, Doyle K. Epidermoid of the cerebellopontine angle. In: Jackler R, Brackmann D. Neurotology. Mosby edit. 1993:823-33.
Talacchi A, Sala F, Alessandrini F, Turazzi S, Bricolo A. Assessment and surgical management of posterior fossa epidermoid tumors: report of 28 cases. Neurosurgery 1998;42:242-52.
Samii M, Tatagiba M, Piquer J, Carcalho G. Surgical treatment of epidermoid cysts of the cerebellopontine angle. J Neurosurg 1996;84:14-9.
Vinchon M, Perturzon B, Lejeune JP, Assaker R, Pruvo JP, Christiaens J. Intradural epidermoid cysts of the cerebellopontine angle: diagnosis and surgery. Neurosurgery 1995;36:52-7.
Partheni M, Constantoyannis C, Liaropoulos K, Sriropoulos P, Tzortzidis F, Maraziotis T. Surgical management of cerebellopontine angle epidermoid cysts. Our experience. In: Sanna M. Acoustic neurinoma and other CPA tumors. Monduzzi editore 1999:773-7.
|
Pro Otology |
Journal Home Contents Preview Next |