|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 3, No 1:26-29 © 2003
All rights reserved. Published by Pro Otology Association
Auditory-Vestibular Disorders in Otobasis Fractures
*K. Tenev, *P. Rouev, *P. Dimov, †J. Toneva, *R. Hristova
*Clinic of Otorhinolaryngology, University Hospital
†Department of Radiology, University Hospital, Trakia University, Stara Zagora, Bulgaria
ABSTRACT
Objective: A series of patients with temporal bone fractures are reviewed to correlate mechanism of injury, fracture location, and outcome.
Study design: A retrospective analysis.
Setting: ENT and Neurosurgery clinics, University Hospital, Stara Zagora
Patients: 80 patients evaluated between 1999 and 2002 for temporal bone fractures was undertaken.
Intervention: Assessment of auditory and vestibular function is reported. Follow up varied from 3 months to 3 years.
Results: A total of 80 temporal bone fractures were reviewed and later re-examined. The results of conventional X-ray, computerised tomography, clinical, otoneurological and audiological findings were analysed. Transverse fractures were associated with severe sensorineural hearing loss while ossicular disruption and persistent conductive hearing loss frequently accompanied longitudinal fractures. Patients with vertigo or dizziness frequently had a good prognosis.
Pro Otology 1: 26-29, 2003
INTRODUCTION
Hearing loss and vestibular dysfunction are common symptoms after head injuries. Proctor et al. (1956), divide the temporal bone and otobasis fractures in three groups - longitudinal, transversal and combined. All of them could include different structures, which depends on the severity of trauma. In 1936 Voss used the term “oblique fractures” and distinguished the following types of fractures:
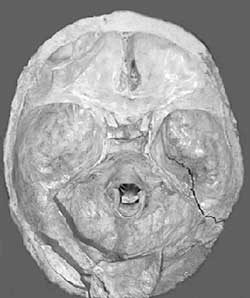
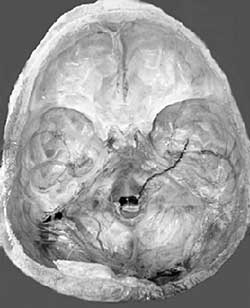
- Longitudinal fractures affecting the middle ear (FIG. 1)
- Transversal fractures affecting the inner ear (FIG. 3)
- Oblique-transversal fractures
- Oblique-longitudinal fractures
- Combined fractures
Dividing the fractures on longitudinal and transversal is only conventional because the line of fracture varies a lot and is often spiral in type. The type of every fracture is determined according to its clinical findings such as otoliquorhea or bleeding from the external auditory meatus, perforation of the tympanic membrane or blood in the middle ear, conductive, sensorineural or mixed hearing loss or nystagmus with/without affecting the cranial nerves. Almost 50% of the cases with fractures of otobasis can’t be visualised with conventional roentgenological examination and CT is needed (Jennet, 1980). The use of high-resolution CT gives the possibility for detailed examination of fracture lines (FIG. 2, 4). The exact course of fracture line could be specified with the use of different sections (coronary and axial).
MATERIAL AND METHODS
A retrospective analysis of patients evaluated between 1999 and 2002 for temporal bone fractures at ENT and Neurosurgery clinics is undertaken. Assessment of auditory and vestibular function is reported. Follow up varied from 3 months to 3 years. 80 patients with temporal bone fracture are investigated.
First an otological evaluation is kneaded and determination of the existence of otoliquorhea. Evaluation of the CN follows, any cerebellar and cerebral dysfunction is lookout, also the existence of nystagmus. Then the state of hearing is determined. Otoneurological investigation is done when the condition of patient is good enough.
The high-resolution CT is a method of choice when specifying the type of the otobasis fractures. The contemporary tomography has a high-resolution possibility at about 0.1 mmі, and the gauge of cuttings is reduced to 1.5 mm.
We’ve used a CT “Siemens” - Somatom ARTX with a special program for the inner ear (gauge of cuttings 2 mm, 130 kV, 3.2 sec., incidence of Gentry +22є parallel to upper surface of pyramid) with high resolution image processing and MPR program for sagital and frontal reconstruction of the image in another projection (Yamaki et al., 1987; Fatterpekar et al., 1999).
RESULTS
| Table 1. Types of otobasis fractures. |
|
A total of 80 temporal bone fractures were examined and later re-examined. All of the patients entered conventional X-ray, computerised tomography, clinical, otoneurological and audiological investigation. The division of fractures according to their type is shown in Table 1.
The typical findings in cases with transversal and longitudinal fracture of the temporal bone are shown on FIG. 3 and 4. Transverse fractures were associated with vertigo, haemotympanum and severe sensorineural hearing loss, while longitudinal fractures frequently were accompanied by traumatic rupture of the tympanic membrane (TRTM), ossicular disruption and persistent conductive hearing loss (Table 2, 3, 4).
We found that 78.05% (32, n=41) of the patients with LFTB and 7.14% (2, n=28) of the patients with TFTB had a TRTM (p<0.0001).
The middle ear is more often affected from longitudinal fractures than the inner ear, which is cut across mainly from transversal fractures (p < 0,0001). The patients with TFTB have more often vertigo or dizziness in comparison with those with LFTB (p<0.039) but the prognosis is good (Table 4).
| Table 2. Relation between fractures of the temporal bone and the otoscopic findings (TRTM –traumatic rupture ot the tympanic membrane; LFTB – longitudinal fractura of temporal bone; OFTB – oblique fractura of temporal bone; TFTB – transversal fractura of temporal bone; CFTB – combined fractura of temporal bone). |

|
| Table 3. Relation between fractures of the temporal bone and those of the external, middle and inner ear according to their currency. |

|
DISSCUSSION
The high-resolution CT is very effective for investigation of the temporal bone. The classification of fractures is made according to the position of the fracture line towards the long axis of pyramid. CT at intervals of 2 mm gives enough information for the routine investigation of the temporal bone. Clausen (1979), Zimmerman (1993), Kahn (2000), recommend the use of CT when a fracture of the temporal bone exists, and MRI when there is a suspicion for liquid in mastoid cells.
Begall (1994) reports that 70% from the investigated patients have longitudinal fractures, 15% have transversal and 15% - with combined fractures. In our study 51% of fractures are longitudinal, 35% - transversal, 10% - combined and 3% are oblique.
| Table 4. Relation between fractures of the temporal bone, type of hearing loss and the existence of vertigo. |
|
The longitudinal fractures of temporal bone (LFTB) arise as a result of direct trauma over the temporo-parietal part of the scull. The fracture line passes the squamous part of the temporal bone forward and down, and through tegmen timpani, the “roof” of the external auditory meatus and middle ear toward foramen lacerum or spinosum. The clinical features include bleeding from the external auditory meatus, perforation of the tympanic membrane and conductive hearing loss. The latter recovers if the auditory chain is intact and if not a surgical treatment is needed lately. The conductive hearing loss over 30 dB two months after trauma is typical when the auditory chain is injured. In 15% of the patients with otobasis fractures we’ve determined damages of the auditory chain. Some authors (Wright and Holland, 1974; Jennet, 1980) found LFTB with the help of axial CT and the canal of the facial nerve with coronary cutting. The CT findings in those fractures include fracture-lines and liquid in mastoid. If incus is luxated, displaced or fractured an “ice-cream” fracture is the resultant in which the malleus looks like ice cream funnel. Also malleus and incus which are normally at a distance from the attic walls could be pathologically dislocated (Wennmo et al., 1993).
The transversal fractures of temporal bone (TFTB) arise after severe indirect traumas over that bone and more often after front-occipital hitting. In such cases the fracture line crosses the long axis of pyramid which is connected with injury of the bony labyrinth, including the vestibule of the inner ear with or without rupture of the tympanic membrane and accompanying noise. The clinical signs in those cases are nystagmus and vertigo, sensorineural-hearing loss with or without paralysis of the facial nerve, haemotympanum and intact tympanic membrane.
Sensorineural hearing loss with noise arises after traumas with or without fractures of otobasis. When a fracture doesn’t exist the injury is a result of the power wave. TFTB are seen well on CT with axial and coronary cutting. The fracture line could pass through the internal auditory meatus, cochlea, vestibule and the semicircular canals and through the facial nerve canal. Schindler and Niparko (1998) thinks that 96 % of the patients with such fractures have hearing loss about 60 dB.
Bechara (1998), supplement to the classification of the fractures of temporal bone the so-called oblique fractures (OFTB). The fracture line in those cases has more horizontal plane than the longitudinal fractures and begins from the backside of squama, passing down the mastoid to the growth of Henle. The fracture divides the external auditory meatus longitudinally into upper and lower halves. The clinical features are similar to those in longitudinal fractures and are best visualised on coronary CT. That’s why we accept the classification of Ghorayeb and Yeakley (1992), which is based on 3-D CT reconstruction. Wennmo et al. (1989), think that more than 2/3 of the patients with FTB have vertigo. The mechanism of its appearing is different and depends on that if the damages are central or peripheral (Wennmo and Svensson, 1989).
CONCLUSION
Hearing trauma after head injury is often due to fractures of otobasis. These fractures are rare strictly longitudinal or transversal, which depends on the mechanism of injury. Bone fragmentation and fracture line varies a lot. Classification and treatment depends on the relation of fracture line to the crest of petrose bone. Longitudinal fractures are the most frequent fractures of otobasis, which affect mainly the middle ear structures and are connected with sensorineural hearing loss. Conductive hearing loss persisting 6 to 7 weeks after trauma and exceeding 30 dB, with otoliquorhea or damage of the facial nerve in its tympanic or mastoid segment is an indication for surgical exploration. Transversal fractures are more rare than longitudinal ones and affect mainly the inner ear, which is connected with sensorineural hearing loss and vertigo. Haemotympanum when tympanic membrane is intact is often in such cases. The combined fractures of otobasis are the most rare seen fractures, which affect not only the middle but also the inner ear.
The vestibular system is not so vulnerable as the auditory system. The vestibular symptoms improved or disappeared in all cases, whereas not infrequently, a sensorineural hearing loss remained.
The CT of otobasis takes the main place in diagnosing the fractures of otobasis. The method is non-invasive with minimal roentgenological charge and gives the possibility for diagnosing fine changes in bone structures.
REFERENCES
Bechara Y. Temporal Bone Fractures: Longitudinal or Oblique. Laryngoscope 1998;102:129-31.
Begall K. Klinische und Katamnesische Untersuchungen nach Otoschaedel Fraktur. HNO 1994;42:405-12.
Clausen C. CT bei frontobasalen Schadelhirnverletzungen. Laryngorhinology 1979;57:697-9.
Fatterpekar GM, Mukherji SK, Lin Y, Alley JG, Stone JA, Castillo M. Normal canals at the fundus of the internal auditory canal: CT evaluation. J Comput Assist Tomogr 1999;23(5):776-80.
Ghorayeb BY, Yeakley JW. Temporal bone fractures: longitudinal or oblique? The case for oblique temporal bone fractures. Laryngoscope 1992;102(2):129-34.
Jennett B. Skull x-rays after recent head injury. Clin Radiol 1980;31:463-9.
Kahn J, Stewart M, Diaz-Marchan P. Acute Temporal Bone Trauma: Utility of High-Resolution Computed Tomography. The American Journal of Otology 2000;21:743-52.
Proctor B, Gurjian E, Webster J. The ear in head trauma. Laryngoscope 1956;66:16-59.
Schindler J, Niparko J. Transverse Temporal Bone Fractures, Arch Otolaryngol Head Neck Surg 1998;124:814-7.
Voss O. Die Chirurgie der Schadelbasis Frakturen auf Grund 25-jahriger Erfarung. Johann Ambrosius Barth Leipzig 1936.
Wennmo C, Spandow O. Fractures of the temporal bone - chain incongruencies. Am J Otolaryngol 1993;14(1):38-42.
Wennmo C, Svensson C. Temporal bone fractures. Vestibular and other related ear sequele. Acta Otolaryngol Suppl 1989;468:379-83.
Wright JWJr, Silf KL. Acoustic and vestibular defects in lightning survivors. Laryngoscope 1974;84:1378-86.
Yamaki T, Yoshino E, Ghorayeb BY. High resolution CT scan of temporal bone fractures: association of facial nerve paralysis with temporal bone fractures. Head Neck Surg 1987;9:162-6.
Zimmerman R, Ganzel T. Peripheral Hearing Loss Fillowing Head Trauma in Children. Laryngoscope 1993;103:87-91.
|
Pro Otology |
Journal Home Contents Preview Next |