|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 2, No 1:8-10 © 2002
All rights reserved. Published by Pro Otology Association
A Newly Designed Stapedotomy Prosthesis
G. Velegrakis, E. Prokopakis, Al. Karatzanis, I. Hajiioannou, Em. Helidonis
Department of Otolaryngology, University of Crete School of Medicine, Heraklion, Greece
ABSTRACT
Objective: The study presents the long-term results of a new homemade stapedotomy prosthesis.
Study Design: This study analyses 42 consecutive cases with a medical follow-up period between eighteen months and five years.
Setting: Department of Otolaryngology, University of Crete School Medicine, Heraklion.
Patients: 42 patients with stapes fixation: 27-femails, 15-males. The mean age - 43,5 years.
Intervention: Preoperative and postoperative pure tone audiograms, speech reception thresholds, discrimination scores were performed. Conventional stapedotomy technique under local anesthesia we performed in all patients.
Main Outcome Measures: Standard audiometric tests. In all patients preoperative air-bone gap (ABG) between 10 and 25 dB HL was found. The average postoperative ABG was 7 dB HL.
Results: After the placement of the prosthesis no early or late postoperative complications (bleeding, vertigo, facial paresis, osicularnecrosis, granuloma formation, tympanic membrane perforation) were observed. Postoperative hearing results are similar to those achieved with other commercially available pistons.
Conclusions: The innovations after a proper and save insertion of the prosthesis into the oval window associated with excellent manipulation and handling. These advantages could be of major importance for younger surgeons and trainees.
Key Words: Otosclerosis, Prosthesis, Stapedotomy.
Pro Otology 1: 8-10, 2002
INTRODUCTION
When stapedectomy procedure with interposition of a stapes piston was introduced in 1958, a new era in the surgical treatment of otosclerosis began (1). Ever since, great efforts have been made towards improving the biomedical properties of the implants as well as the surgical technique itself (2,3). Although stapedectomy, involving the removal of stapes completely, was the initial surgical technique, it has largely been replaced today by the stapedotomy or small fenestra method (4,5,6). The use of Laser in stapes surgery has also been introduced as an attempt to improve surgical efficiency (7,8).
The main differences in the design of stapes prostheses are focused at both ends of the implant. A number of different designs have been proposed and used for prosthesis attachment to the incus (2). Several designs are also used to improve transmission of sound through the oval window to the inner ear (2). Inspite the numerous innovations regarding the design of stapes prostheses, issues that concern safety against shaft intrusion through the oval window and decreased visibility during piston placement are always under consideration.
Our Department has previously presented a preliminary report of a newly designed stapedotomy prosthesis, which offers solutions to stapes fixation associated with otosclerosis (9). This study reports the long-term results of our experience with stapedotomy using the new prosthesis.
PATIENTS AND METHODS
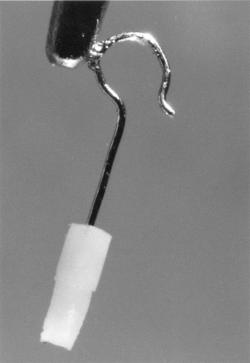
The prototype prosthesis was designed by the first author and manufactured by Smith & Nephew Richards Inc., Memphis, Tenn., USA (commercial name 'Velegrakis Piston') (Figure 1). The innovations of the new prosthesis concern both portions, design for attachment to the incus and shaft (9). The platinum wire has been reconfigured into a standard round wire with a flattened tab enabling easier grasping and positioning of the piston. The fluoroplastic shaft is reconfigured into a single shaft with two different diameters. The stepped-down design is intended to enhance visualization and reduce the chance of the implant protruding into the vestibule.
There are several choices of prosthesis length, ranging from 3.75 mm to 5.00 mm, in order to accommodate differences in the size of the stapes and to eliminate the need to trim.
Our series include a total number of 42 individuals with stapes fixation, operated using the new prosthesis, during the last five years. Twenty-seven patients were females and 15 were males. The mean age of the entire group was 43.5 years. Conventional stapedotomy technique under local anesthesia, was performed in all patients. The stapes fixation was confirmed intraoperatively in every case. Prosthesis length ranged between 4.25 mm and 4.75 mm, while the shaft's diameter ranged from 0.4 mm to 0.6 mm in all cases (Table 1). Postoperative follow-up period ranged from eighteen months up to five years.
Standard preoperative and postoperative audiometric tests, including pure-tone audiograms, speech reception threshold and discrimination scores were performed on all patients using calibrated equipment in a soundproof room. Preoperative and postoperative air and bone hearing levels were determined by calculating the respective pure tone averages at 500, 1000, 2000 and 4000 Hz. The air-bone gap (ABG), used to report hearing results was defined as the difference between the postoperative air-hearing level and the preoperative bone-hearing level. In all cases, a preoperative air-bone gap between 10 and 25 dB HL was found. All patients showed preoperative hearing levels worse than 40 dB HL.
RESULTS
After the placement of the prosthesis, no early or late postoperative complications, such as bleeding, vertigo, facial paresis, ossicular necrosis, granuloma formation and tympanic membrane perforation were observed. No early or late sensorineural hearing loss has been seen in any patient to date.
In our series, the average postoperative ABG was 7 dBHL in frequencies between 250 Hz and 4 kHz (ranging from 3 to 22 dB HL). Air-bone gap closure within 10 dB HL was observed in 35 patients (83.3%). Six patients showed ABG closure between 10 and 20 dB HL (14.2%). In a single case ABG closure was 22 dB HL. Postoperative hearing results showed no statistical difference between pistons of different length and/or shaft diameter.
DISCUSSION
Among the different implants that have been used in stapes surgery, variations exist in size, shape, weight and mass. All previous parameters should add up to create an ideal stapes prosthesis. This would be one that exerts no mass on the inner ear at rest, and its weight would be similar to that of the normal stapes (2). Another issue to be addressed is the type of material the prosthesis is made of and its consequent interaction with host tissue. Currently available prostheses are most commonly composed of three materials: a Teflon-type polymer, stainless steel, or platinum (2). These are nonreactive and non-ferromagnetic materials. Polyethylene, is no longer utilised because of its reaction with middle ear tissue (2). Other materials, like pure gold, have also been proposed. At present, the most commonly employed prostheses in stapes surgery are the total Teflon or teflon wire pistons (2).
So far, despite the numerous innovations concerning prosthesis design, important issues still under consideration involve safety against shaft intrusion through the oval window with consequent labyrinthine trauma, as well as decreased visibility during prosthesis insertion. Lack of a specially designed handling portion on most commercially available prostheses, results in manipulation difficulties during piston insertion, thus prolongating the operation time. Moreover, when stapedotomy is undertaken, the cylinder-like shape of most piston shafts does not provide a mechanism preventing intrusion of the prosthesis through the oval window. Thus, consequent injury to the membranous labyrinth, either intraoperatively or postoperatively, can occur.
The new prosthesis offers significant advantages due to its specially designed handling portion and the stepped-down design of its shaft. The created 'tab' on the platinum ribbon helps the surgeon to easily grasp and handle the prosthesis with an ear forceps (Figure 1). This design increases visualisation during placement of the piston into the oval window. No further manipulations are needed, and there is no actual risk of tympanic membrane perforation or other complications due to the position and size of the tab. If the surgeon decides not to use an ear forceps for piston positioning, the tab would not create any manipulation difficulties, although the advantage from its potential use would be lost. Such a concept is of minor importance to the experienced surgeon, but it certainly enhances the surgical ability of a younger trainee. At the same time, this innovation enables an excellent manipulation of the prosthesis, and the opportunity for the surgeon to exert his technical skills resulting in a safe and time-saving procedure.
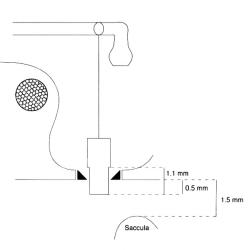
The stepped-down design of the new prosthesis shaft reduces the chance of labyrinthine trauma during or after stapedotomy (Figure 2). During the procedure, the thinner bottom portion of the shaft is positioned properly through a fenestra created at the footplate, while the wider upper portion is prevented from entering through the fenestra. The narrower bottom portion results in safe placement of the prosthesis, without intraoperative injury to the membranous labyrinth. Such a risk is greater for the inexperienced surgeon where the use of this newly designed shaft is more advantageous. More speciffically, the prosthesis would not protrude through the fenestra for more than 1.10 mm, which is the length of the narrower bottom portion, while the shorter distance between the inner surface of the footplate and the membranous labyrinth is approximately 1.5 mm. It is noted that these dimensional relations are realistic with regard to the posterior part of the footplate which is the peferred site for fenestration. In addition, and due to the stepped-down shaft design, postoperative sharp intrusion of the prosthesis into the vestibule during loud sound irritations, although rare in any case, is also avoided.
If the opening of the fenestra is 0.4 or 0.6 mm, so that the corresponding prosthesis can be placed, the need for seal in order to create a watertight closure is avoided. In our experience, placement of a blood clot around the fenestra, has prooved to be sufficient as a seal. Moreover, manual testing of piston mobility, following placement, by back and forth movement of the long process of the incus, can be performed in order to exclude the possibility of increased friction with a corresponding attenuation of the acoustical vibrations. Up to now, after using this piston for 5 years, we have no patients with symptoms associated with perilymphatic fistula due to the lack of seal.
Postoperative hearing results following implantation of the new piston are similar to those achieved with other commercially available pistons (6,10). Air-bone gap closure within 10 dB HL was observed in 83.3% of cases in our series. Only a single patient, in our group, failed to show significant postoperative hearing benefit.
In conclusion, we believe that our innovations permit a proper and safe insertion of the prosthesis into the oval window in addition with excellent manipulation and handling of the implant, resulting in a time-saving operation. The postoperative results are equal to those of other commercially available prostheses. Maximum visualization of the surgical field is achieved, while the stepped-down design of the shaft prevents the prosthesis from protruding into the vestibule.
Shea JJ Jr. Fenestration of the oval window. Ann Otol Rhinol Laryngol 1958;67:932-51.
Slattery WH III, House JW. Prosteses for stapes surgery. Otolaryngol Clin North Am 1995;28(2):253-64.
Treace HT. Biomaterials in ossiculoplasty and history of development of prostheses for ossiculoplasty. Otolaryngol Clin of North Am 1994;2(4):655-62.
Rizer FM, Lippy WH. Evolution of techniques of stapedectomy from the total stapedectomy to the small fenestra stapedectomy. Otolaryngol Clin of North Am 1995;28(2):443-51.
Kursten R, Schneider B, Zrunek M. Long term results after stapedectomy versus stapedotomy. Am J Otol 1994;15:804-6.
Levy R, Shvero J, Hadar T. Stapedotomy technique and results: ten years' experience and comparative study with stapedectomy. Laryngoscope 1990;100:1097-9.
Nissen RL. Argon Laser in difficult stapedotomy cases. Laryngoscope 1998;108:1669-73.
Lesinski SG, Newrock R. Carbon dioxide Lasers for otosclerosis. Otolaryngol Clin of North Am 1995;28(2):417-36.
Velegrakis GA, Papadakis CE, Prokopakis EP, Helidonis ES. A new stapedotomy prosthesis: Preliminary report. ORL 1999;61:6-9.
Persson P, Harder H, Magnuson B. Hearing results in otosclerosis surgery after partial stapedectomy, total stapedectomy and stapedotomy. Acta Otolaryngol (Stockh) 1997;117:94-9.
|
Pro Otology |
Journal Home Contents Preview Next |