|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 4, No 2-3:8385 © 2004
All rights reserved. Published by Pro Otology Association
Simplified Combinated Operative Approach to the Middle Ear for Cochleostomia of the Promontorium at the Cochlea Implants System Med El
Ivan Tzenev
ENT Clinic, University Hospital Tsarisa Joanna, Sofia, Bulgaria
ABSTRACT
Objective: A combinated surgical access to the inner ear for cochleostomia which matches endochannel and trnsmastoidal approachis is described.
Setting: Clinic of ORL, Tsarisa Joanna Hospital, Sofia.
Interventions: Modification of cochlear implantation.
Conclusion: The presented method is extremely simple. It hides no danger of injury of the facial nerve, saves surgical time and allows a quick implanting of the electrode in the cochlea.
Key words: Cochlear implantation, Alternative surgical approaches.
Pro Otology 2-3:8385, 2004
Introduction
In the last years the cochlear implantation incessantly imposes as an hearing improving method without alternative as far as prelingual and postlingual deaf patients are concerned. About 45 systems of the firm Med El have been implanted mainly at children till that moment in Bulgaria. The postoperative and hearing results are very good.
All this lot predetermines the improvements in the surgical techniques we used to apply in the opening stages of introducing the cochlear implanting. Now we have elaborated and apply a simplified fast safety combinated technique which saves the operative time and diminishes the risk for facial nerve injury. In a previous publication of ours we demonstrate the so called parachannel access to the middle ear (1). To accomplish this we remove a part of the mastoid, keeping close to the back wall of the outer auditory channel and the cochleostomia is performed through the channel. For this purpose a removement of a part of the channel wall till visualizing tendo m. stapedii, in the way it is done at the approach for otosclerosis, is done in advance.
|
|
material and methods
The operation is performed under general anesthesia with additional local infiltration of Lidocain and Adrenalin for decreasing the bleeding. The retroauricularl skin section is done and resembles the Wildes one, but it is closer to the retroauricular flap in accordance with the metal pattern (FIG. 1). The section reaches the periost, after which with an elevator a modo Friere the periost is released from planum mastoideum and a part of the posterior channel wall (FIG. 2). At the height of spina meati acustici externa a horizontal section on the back part of the channel skin is done and the auricular is dragged out forward through the opening by a lint band (FIG. 3). With a vertical knife a modo Plester two parallel sections of the channel wall at the level of annulus fibrosus till the place of horizontal section are performed and after that the skin is removed till the level of annulus fibrosusby means of a elevator. Carefully we disconnect and push forward chorda tympani and after that by a curette or borer take down a part of the back channel wall until the tendon of m. stapedius is seen (FIG. 4).
|
|
|||||
|
|
The operation continues with taking off the bone structure from planum mastoideum close to the channel wall orientated to the tendon of m. stapedius and in a depth about 1 cm when children are concerned and 1,5 cm at grown-ups we reach the long processus of the incus, the promontorium respectively (FIG. 5). In this part of the promontorium between the two windows in an oblique direction by means of a diamond borer 0.6 mm we perform the cochleostomia, which is extended till about 1.3 - 1.6 mm progressively. This is where the active electrode goes through (FIG. 6).
|
|
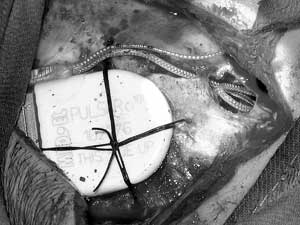
FIG. 7. It fixes the implant with threads. |
The rest part - forming the recipients (implants) bed, follows the well-known and established from the daily practice techniques. Compulsorily we fix the implant with threads Vicril 3-0 in four or five points. (FIG. 7) This creates the necessitive comfort for the electronical part remaining implanted under the skin.
conclusion
The proposed combinated method for economical bone access to the structures of the middle ear with bilateral approach is easily performed technically. It has no hidden risks for the facilal nerv, safe time and anesthetics.
REFERENCES
Tzenev Iv, K. Kunev. Surgical Approaches for Cochlear Implantation. ProOtology 2003(3);2 Suppl.:33-35.
|
Pro Otology |
Journal Home Contents Preview Next |





