|
|
Journal Home Contents Preview Next |
Pro Otology
Balkan Journal of Otology & Neuro-Otology, Vol. 4, No 2-3:98100 © 2004
All rights reserved. Published by Pro Otology Association
Blast Injury of the Ear: Our Experience
V. Tzvetkov, H. Zlatanov, M. Spahieva
ENT Department, Military Medical Academy, Sofia, Bulgaria
ABSTRACT
Objective: Patients with damages of eardrum due to blast injury when defects are large in size are subjected to operation. Watch and wait strategy is applied for patients with small lesions when spontaneous healing is possible. The question which time for operation is a proper one is an object for discussion. In the recent paper we share our experience of 15 patients with middle to severe lesions of membranes due to blast injury, who underwent an early operation. We compared them with a control group of 8 patients who were not operated.
Study Design: The study design is a retrospective review.
Setting: ENT Department, Military Medical Academy, Sofia, Bulgaria
Patients: 15 patients over 18 years old with middle to severe bilateral and unilateral perforation of tympanic membrane.
Material and Methods: A material from tragus cartilage with the size of tympanic membrane was used for correction of perforations. We used endaural incision. Pollution due to blast injury required lavages of tympanic cavity. Traumatic margins of operation were excised and adequately treated. Examination of tympanic cavity showed different damages of ossicular system, lack of ossicles (only stapes remained in 3 patients), rearrangements and fractures of manubrium and/or incus. After the reconstruction of ossicular system we placed graft to the cavity. This method would reduce adhesions.
Results: Data from microscopic otoscopy after detamponading between the 14-th and the 16-th day showed good engraftment and initial vascularisation in all but 2 patients.
Key words: Tympanoplasty, Blast injuries.
Pro Otology 2-3:98100, 2004
INTRODUCTION
The necessity of operation of traumatic lesions of tympanic membrane due to blast injury is still questionable. Watch and wait strategy is a proper one referring to small perforations because of tendency of spontaneous healing in most of the cases. Opinions on the proper time for operation of total/subtotal defects differ a lot. In the recent paper we discuss the effect of early tympanoplasty (up to 72 hours after the trauma) for the treatment of severe lesions of tympanic membrane in comparison with the control group unoperated patients.
METHODS
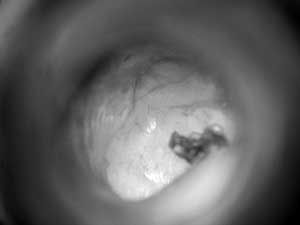
Fifteen patients over 18 years old with middle to severe bilateral and unilateral perforation of tympanic membrane and different damages of structures of tympanic cavity as a result of blast injury have been undergone an early tympanoplasty for the recent 3 years. The control group consisted of 8 patients with unilateral perforations of tympanic membrane comprising approximately 40% of its area. Our strategy in these cases was watch and wait with antibiotics and neurotropic therapy. According to the extent of blast injury and the distance to it patients suffered different accompanying side effects: thermal effects, suffusions on face and ears. Microscopic otoscopy demonstrated bilateral total perforations of tympanic membrane in 4 patients; bilateral subtotal perforations- in 5 patients; subtotal defect of unilateral tympanic membrane- in 2 patients; bilateral membrane lesions comparising 30- 40% of the area and unilateral membrane lesions of the same kind- in 2 patients. Pollutions of dust and fragments of the surface of external auditory meatus and membrane were seen in all cases. Preoperative audiograms gave data of combined decrease of hearing ability up to deafness in 11 of heavily injured patients; decrease of hearing ability- in 4 patients and the control group. Patients had typical complaints of a noise of high tonality in both ears. Three of the most heavily injured patients suffered periodically vertigo, nausea and profuse sweating. These symptoms were effectively treated by neurotropic and vasodilatative drugs. Patients were consulted by neurologist, neurosurgeon and anaesthesiologist and operated up to 72 hours after the trauma.
General endotracheal anaesthesia was applied. A material from tragus cartilage with the size of tympanic membrane was used for correction of perforations. We used endaural incision. Pollution due to blast injury required lavages of tympanic cavity. Traumatic margins of operation were excised and adequately treated. Examination of tympanic cavity showed different damages of ossicular system, lack of ossicles (only stapes remained in 3 patients), rearrangements and fractures of manubrium and/or incus. After the reconstruction of ossicular system we placed graft to the cavity. This method would reduce adhesions. Auditory meatus has been tamponated for 14 days. All patients have been treated with pre- and postoperatively with antibiotics, intravenous infusions with vasodilatators, vitamins and neurotropic drugs useful for the perceptive component of hearing damage for 10 days.
|
|
RESULTS
Data from microscopic otoscopy after detamponading between the 14-th and the 16-th day showed good engraftment and initial vascularisation in all but 2 patients. In one of them a small defect in inferior anterior segment remained and necessitated a reoperation after 3 months; in the other patient- a fissure- like perforation was diagnosed in anterior superior quadrant but after treatment with Vagothyl it was healed spontaneously for approximately 15 days.
Microscopic otoscopy in the control group on the 15-th day after the trauma showed a decrease in size of perforation in 3 patients; the size of lesions with typical hypotrophic changes of the margins remained the same in 2 cases and in 3 patients a complication was diagnosed- inflammation of the membrane with suppuration requiring therapy with antibiotic ear drops. Examination on the 30-th day after the trauma showed healing of the perforation in the 2 patients. The lesions were extended up to 40- 50% of the size of pars tensa in the 2 patients, 2 patients from the control group were operated successfully after 60 days. Audiometric examination was provided preoperatively and approximately 30 days after the operation. Audiometric examination of 6 of most injured patients after the treatment undergo significant hearing improvement with reduced cochlear gap and perceptional hearing decrease for frequency over 4000 Hz. Audiograms of the control group on the 30-th day after the trauma demonstrated full hearing restoration in the patients with healing of the perforation. In the remaining cases examination proved normal perceptional abilities but preservation of conductive deficiency without changes in cochlear gap.
DISCUSSION
Ear is extremely sensitive to detonation and sound waves due to blast injury that explains why the damages of tympanic membrane of middle and outer ear are one of the most frequent traumas at blast injuries (1,2) High air pressure causes also fractures and disarrangement of ossicular system with/ without trauma of windows (oval and round). Air pressure over 35 kPa causes perforation in over 50% of population (3). High percentage of spontaneous healing (approximately in 70- 80% of cases) (4) is a reason why some authors watch and wait for an operation. But our experience shows that a delay of operation is a correct strategy for the treatment of only small defects of membrane not larger than a quarter of its size. An operation- tympanoplasty of the cavity and a reconstitution of ossicular system when needed are almost always necessary. The proper time for an operation is still questionable (5). In our opinion patients should be operated as soon as possible after the trauma if contraindications are absent. This approach reduces the possibility of passing an infection from auditory meatus to the middle ear. Antibiotic lavages during operation and 7 days treatment with antibiotics after the operation are used for prophylaxis. Fragments from epithelium of auditory meatus and membrane eventually placed in the tympanic cavity may cause cholesteatoma after the spontaneous healing. The margins of the defect with the remaining parts of membrane are tucked to the cavity and in early operation part of them can be rearranged to lessen the size of the defect. Such grafts facilitate the operation.
CONCLUSSIONS
In our opinion the early tympanoplasty used for the treatment of traumatic perforations of tympanic membrane spreading over 1/3 of its size is reasonable because:
Inflammation comlplications of tympamic cavity are avoided;
A revision of tymppanic cavity and ossicular system is possible before adhesions have been formed (necessary condition for successful treatment and better restoration);
Postraumatic hypotrophy of membrane is avoided ensuring successful results from the treatment.
REFERENCES
Walsh RM, Pracy JP, Huggon AM, Gleeson MJ. Bomb blast injuries to the ear: the London Bridge incident series. J Accid Emerg Med 1995;12:194-8.
Wolf M, Ben-Shoshan J, Kronenberg J, Roth Y. Blast injury of the ear. Mil Med 1991;156:651-3.
Kerr AG, Byrne JE. Concussive effects of bomb blast on the ear. J Laryngol Otol 1975; 89:131-43.
prem N, Branica S, Suboti
prem N, Branica S, Dawidowsky K. Tympanoplasty after War Blast Lesions of the Eardrum: Retrospective Study. Croat Med J 2001;42:642-5.
|
Pro Otology |
Journal Home Contents Preview Next |